Myanmar Oxford Clinical Research Unit, Yangon, Myanmar.
Nuffield Department of Medicine, Centre for Tropical Medicine and Global Health, University of Oxford, Oxford, UK.
Drugs. 2018 Jun;78(9):861-879. doi: 10.1007/s40265-018-0911-9.
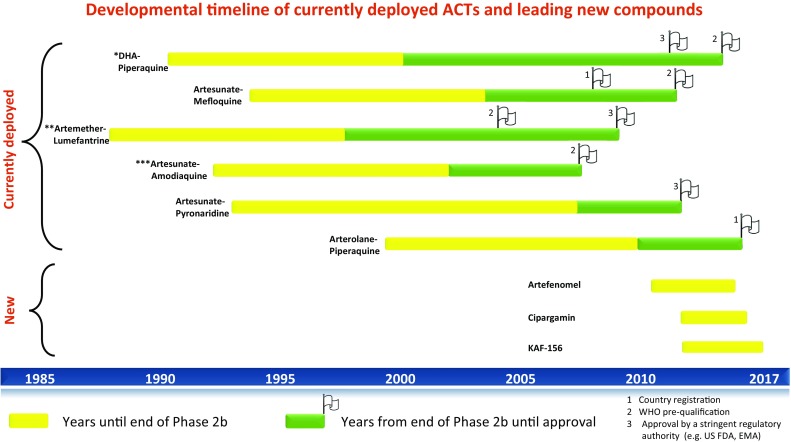
The last two decades have seen a surge in antimalarial drug development with product development partnerships taking a leading role. Resistance of Plasmodium falciparum to the artemisinin derivatives, piperaquine and mefloquine in Southeast Asia means new antimalarials are needed with some urgency. There are at least 13 agents in clinical development. Most of these are blood schizonticides for the treatment of uncomplicated falciparum malaria, under evaluation either singly or as part of two-drug combinations. Leading candidates progressing through the pipeline are artefenomel-ferroquine and lumefantrine-KAF156, both in Phase 2b. Treatment of severe malaria continues to rely on two parenteral drugs with ancient forebears: artesunate and quinine, with sevuparin being evaluated as an adjuvant therapy. Tafenoquine is under review by stringent regulatory authorities for approval as a single-dose treatment for Plasmodium vivax relapse prevention. This represents an advance over standard 14-day primaquine regimens; however, the risk of acute haemolytic anaemia in patients with glucose-6-phosphate dehydrogenase deficiency remains. For disease prevention, several of the newer agents show potential but are unlikely to be recommended for use in the main target groups of pregnant women and young children for some years. Latest predictions are that the malaria burden will continue to be high in the coming decades. This fact, coupled with the repeated loss of antimalarials to resistance, indicates that new antimalarials will be needed for years to come. Failure of the artemisinin-based combinations in Southeast Asia has stimulated a reappraisal of current approaches to combination therapy for malaria with incorporation of three or more drugs in a single treatment under consideration.
过去二十年中,抗疟药物的研发呈井喷式增长,产品研发伙伴关系发挥了主导作用。东南亚恶性疟原虫对青蒿素衍生物、哌喹和甲氟喹的耐药性意味着急需新的抗疟药物。目前至少有 13 种药物处于临床开发阶段。其中大多数是用于治疗无并发症恶性疟的血裂殖体杀灭剂,正在进行单一药物或两药联合治疗的评估。处于研发后期的主要候选药物有阿替法尔-亚铁喹和青蒿琥酯-卡法根,均处于 2b 期临床试验阶段。严重疟疾的治疗仍然依赖两种具有悠久历史的注射用药物:青蒿琥酯和奎宁,而 sevuparin 正在作为辅助治疗药物进行评估。特非那喹正在接受严格的监管机构审查,以批准其作为预防间日疟复发的单剂量治疗药物。这是相对于标准的 14 天伯氨喹方案的一项进步;然而,葡萄糖-6-磷酸脱氢酶缺乏症患者发生急性溶血性贫血的风险仍然存在。对于疾病预防,一些新的药物具有潜在的作用,但在未来几年内,不太可能推荐将其用于孕妇和幼儿等主要目标人群。最新预测显示,未来几十年疟疾负担仍将居高不下。这一事实,加上抗疟药物因耐药性而反复失效,表明未来几年仍需要新的抗疟药物。青蒿素类复方药物在东南亚的失败,促使人们重新评估当前的疟疾联合治疗方法,考虑将三种或更多药物纳入单一治疗方案。