Infectious Diseases & Immunity, Imperial College London, Wellcome Trust Imperial College Centre for Global Health Research, London, UK.
Innovación Por la Salud Y Desarrollo (IPSYD), Asociación Benéfica PRISMA, Lima, Perú.
Trop Med Int Health. 2018 Aug;23(8):850-859. doi: 10.1111/tmi.13087. Epub 2018 Jun 22.
Mobile phone interventions have been advocated for tuberculosis care, but little is known about access of target populations to mobile phones. We studied mobile phone access among patients with tuberculosis, focusing on vulnerable patients and patients who later had adverse treatment outcomes.
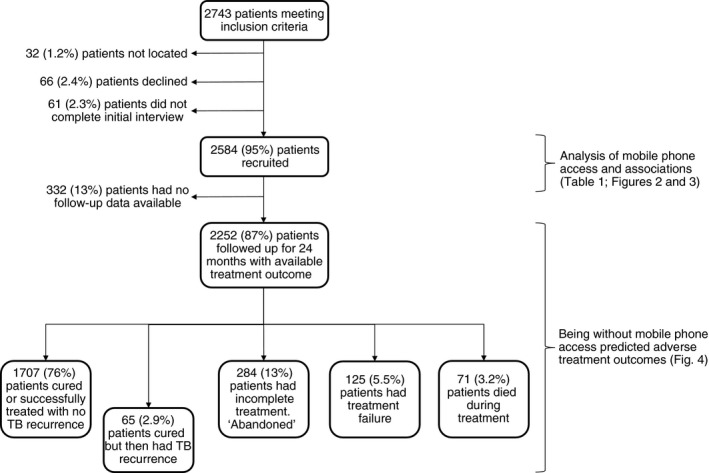
In a prospective cohort study in Callao, Peru, we recruited and interviewed 2584 patients with tuberculosis between 2007 and 2013 and followed them until 2016 for adverse treatment outcomes using national treatment registers. Subsequently, we recruited a further 622 patients between 2016 and 2017. Data were analysed using logistic regression and by calculating relative risks (RR).
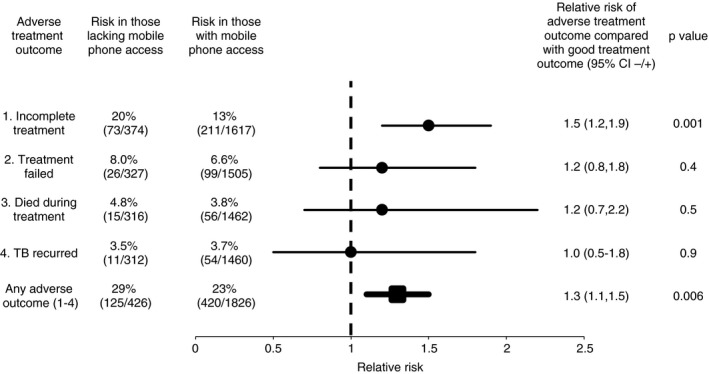
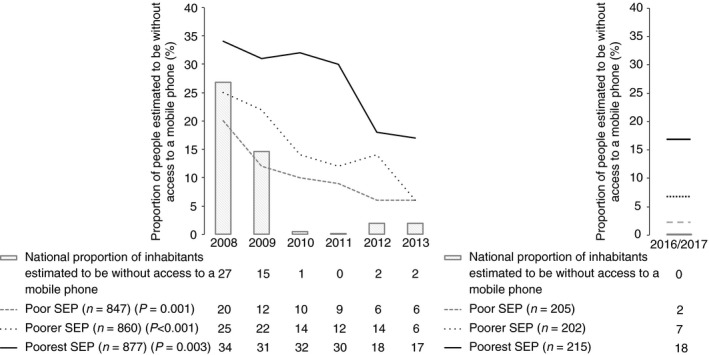
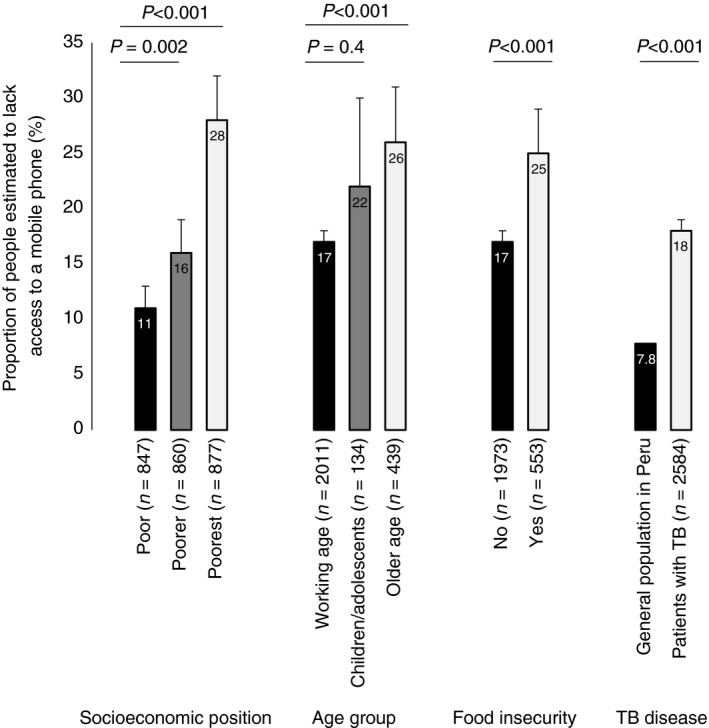
Between 2007 and 2013, the proportion of the general population of Peru without mobile phone access averaged 7.8% but for patients with tuberculosis was 18% (P < 0.001). Patients without access were more likely to hold a lower socioeconomic position, suffer from food insecurity and be older than 50 years (all P < 0.01). Compared to patients with mobile phone access, patients without access at recruitment were more likely to subsequently have incomplete treatment (20% vs. 13%, RR = 1.5; P = 0.001) or an adverse treatment outcome (29% vs. 23% RR = 1.3; P = 0.006). Between 2016 and 2017, the proportion of patients without access dropped to 8.9% overall, but remained the same (18%) as in 2012 among the poorest third.
Access to mobile phones among patients with tuberculosis is insufficient, and rarest in patients who are poorer and later have adverse treatment outcomes. Thus, mobile phone interventions to improve tuberculosis care may be least accessed by the priority populations for whom they are intended. Such interventions should ensure access to mobile phones to enhance equity.
移动电话干预措施已被提倡用于结核病护理,但对于目标人群对移动电话的获取情况知之甚少。我们研究了结核病患者的移动电话获取情况,重点关注弱势群体和随后治疗结果不良的患者。
在秘鲁卡亚俄进行的一项前瞻性队列研究中,我们在 2007 年至 2013 年间招募并采访了 2584 名结核病患者,并通过国家治疗登记册跟踪他们,直到 2016 年出现不良治疗结果。随后,我们在 2016 年至 2017 年间又招募了 622 名患者。使用逻辑回归和计算相对风险(RR)进行数据分析。
2007 年至 2013 年间,秘鲁总人口中没有移动电话的比例平均为 7.8%,但结核病患者的比例为 18%(P<0.001)。没有移动电话的患者更有可能处于较低的社会经济地位,面临粮食不安全问题,年龄超过 50 岁(所有 P<0.01)。与有移动电话的患者相比,招募时没有移动电话的患者随后更有可能出现治疗不完整(20%比 13%,RR=1.5;P=0.001)或治疗结果不良(29%比 23%,RR=1.3;P=0.006)。2016 年至 2017 年间,整体患者中没有移动电话的比例下降到 8.9%,但最贫困的三分之一人群中的比例(18%)与 2012 年相同。
结核病患者中移动电话的获取情况不足,在较贫困且随后治疗结果不良的患者中最为罕见。因此,旨在改善结核病护理的移动电话干预措施可能最无法覆盖到其目标人群。这些干预措施应确保获得移动电话,以增强公平性。