Gray Chancellor F, Prieto Hernan A, Duncan Andrew T, Parvataneni Hari K
Department of Orthopaedics and Rehabilitation, University of Florida, Gainesville, FL, USA.
Arthroplast Today. 2018 Mar 21;4(2):221-226. doi: 10.1016/j.artd.2018.02.002. eCollection 2018 Jun.
Total joint arthroplasty (TJA) remains the highest expenditure in the Centers for Medicare and Medicaid Services (CMS) budget. One model to control cost is the Comprehensive Care for Joint Replacement (CJR) model. There has been no published literature to date examining the efficacy of CJR on value-based outcomes. The purpose of this study was to determine the efficacy and sustainability of a multidisciplinary care redesign for total joint arthroplasty under the CJR paradigm at an academic tertiary care center.
We implemented a system-wide care redesign, affecting all patients who underwent a total hip or total knee arthroplasty at our academic medical center. The main study outcomes were cost (to CMS), discharge destination, complications and readmissions, and length of stay (LOS); these were measured using the 2017 initial CJR reconciliation report, as well as our institutional database.
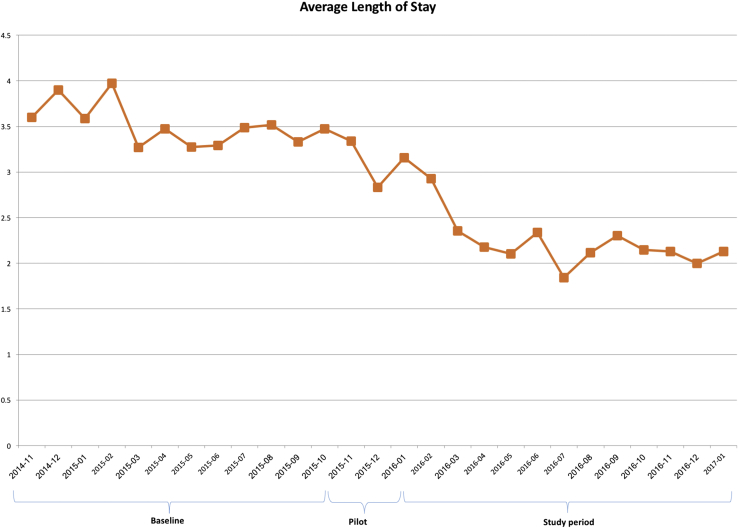
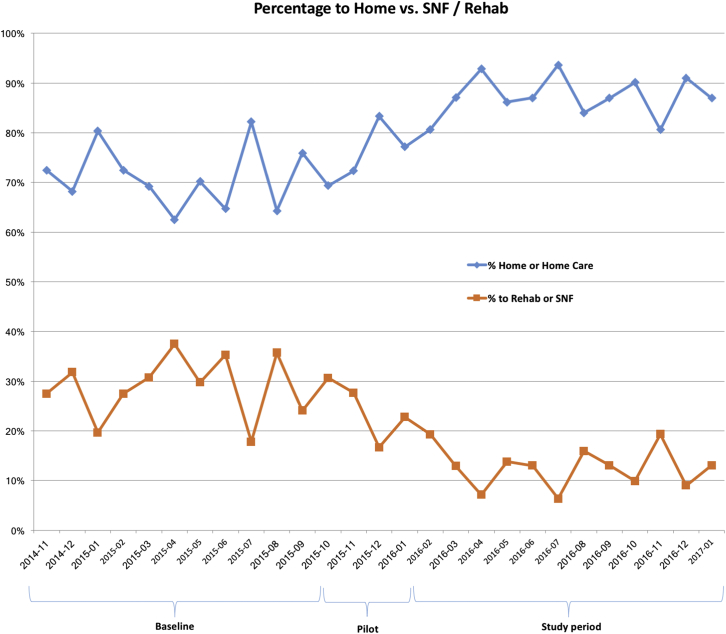
The study included 1536 patients (41% Medicare). Per-episode cost to CMS declined by 19.5% to 11% below the CMS-designated national target. Home discharge increased from 62% to 87%. CMS readmissions declined from 15% to 6%; major complications decreased from 2.3% to 1.9%; and LOS declined from 3.6 to 2.1 days.
A mandatory episode-based bundled-payment program can induce favorable changes to value-based metrics, improving quality and outcomes for health-care consumers. Quality and value were improved in this study, evidenced by lower 90-day episode cost, more home discharges, lower readmissions and complications, and shorter LOS. This approach has implications not just for CMS, but for private payers, corporate health programs, and fixed-budget health-care models.
全关节置换术(TJA)仍是医疗保险和医疗补助服务中心(CMS)预算中支出最高的项目。一种控制成本的模式是关节置换综合护理(CJR)模式。迄今为止,尚无已发表的文献研究CJR对基于价值的结果的疗效。本研究的目的是确定在学术性三级医疗中心的CJR范式下,全关节置换术多学科护理重新设计的疗效和可持续性。
我们实施了全系统的护理重新设计,影响了在我们学术医疗中心接受全髋关节或全膝关节置换术的所有患者。主要研究结果包括成本(对CMS而言)、出院目的地、并发症和再入院情况以及住院时间(LOS);这些数据使用2017年初始CJR核对报告以及我们的机构数据库进行测量。
该研究纳入了1536名患者(41%为医疗保险患者)。CMS的每次发作成本下降了19.5%,比CMS指定的全国目标低11%。家庭出院率从62%提高到87%。CMS再入院率从15%下降到6%;主要并发症从2.3%下降到1.9%;住院时间从3.6天下降到2.1天。
强制性的基于发作的捆绑式支付计划可以促使基于价值的指标发生有利变化,改善医疗消费者的质量和结果。本研究中质量和价值得到了改善,90天发作成本降低、家庭出院增多、再入院和并发症减少以及住院时间缩短证明了这一点。这种方法不仅对CMS有影响,对私人支付者、企业健康计划和固定预算医疗模式也有影响。