McMeekin Peter, White Philip, James Martin A, Price Christopher I, Flynn Darren, Ford Gary A
Institute of Health and Society, Newcastle University, Newcastle Upon Tyne, UK.
2Faculty of Health and Life Sciences, Northumbria University, UK.
Eur Stroke J. 2017 Dec;2(4):319-326. doi: 10.1177/2396987317733343. Epub 2017 Oct 4.
Endovascular thrombectomy is a highly effective treatment for acute ischemic stroke due to large arterial occlusion. Routine provision will require major changes in service configuration and workforce. An important first step is to quantify the population of stroke patients that could benefit. We estimated the annual UK population suitable for endovascular thrombectomy using standard or advanced imaging for patient selection.
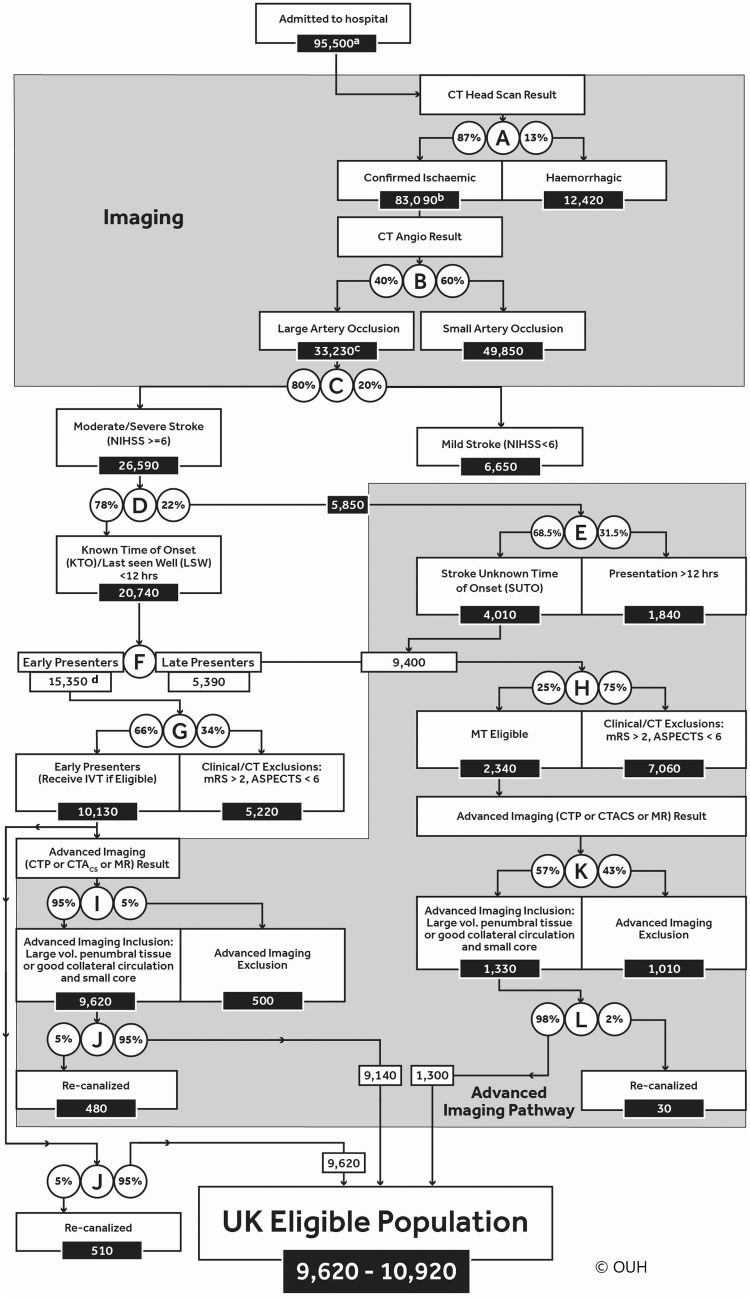
Evidence from randomised control trials and national registries was combined to estimate UK stroke incidence and define a decision-tree describing the endovascular thrombectomy eligible population.
Between 9620 and 10,920 UK stroke patients (approximately 10% of stroke admissions) would be eligible for endovascular thrombectomy annually. The majority (9140-9620) would present within 4 h of onset and be suitable for intravenous thrombolysis. Advanced imaging would exclude 500 patients presenting within 4 h, but identify an additional 1310 patients as eligible who present later.
Information from randomised control trials and large registry data provided the evidence criterion for 9 of the 12 decision points. The best available evidence was used for two decision points with sensitivity analyses to determine how key branches of the tree affected estimates. Using the mid-point estimate for eligibility (9.6% of admissions) and assuming national endovascular thrombectomy coverage, 4280 patients would have reduced disability.
A model combining published trials and register data suggests approximately 10% of all stroke admissions in the UK are eligible for endovascular thrombectomy. The use of advanced imaging based on current published evidence did not have a major impact on overall numbers but could alter eligibility status for 16% of cases.
血管内血栓切除术是治疗因大动脉闭塞所致急性缺血性卒中的一种高效疗法。常规开展此项治疗将需要对服务配置和工作人员进行重大调整。重要的第一步是对可能受益的卒中患者群体进行量化。我们使用标准或先进影像技术来筛选患者,从而估算出英国每年适合接受血管内血栓切除术的人群数量。
综合随机对照试验和国家登记处的数据,以估算英国的卒中发病率,并确定一个描述适合血管内血栓切除术患者群体的决策树。
英国每年有9620至10920名卒中患者(约占卒中住院患者的10%)适合接受血管内血栓切除术。其中大多数患者(9140 - 9620名)会在发病后4小时内就诊,适合接受静脉溶栓治疗。先进影像技术将排除4小时内就诊的500名患者,但会额外识别出1310名就诊较晚但适合手术的患者。
随机对照试验和大型登记数据中的信息为12个决策点中的9个提供了证据标准。对于两个决策点,使用了现有最佳证据并进行敏感性分析,以确定决策树的关键分支如何影响估算结果。采用适合手术的中点估算值(占住院患者的9.6%)并假设全国范围内都能进行血管内血栓切除术,4280名患者的残疾程度将会减轻。
一个结合已发表试验和登记数据的模型表明,英国所有卒中住院患者中约有10%适合接受血管内血栓切除术。根据当前已发表的证据使用先进影像技术,对总体数量没有重大影响,但可能会改变16%病例的适合手术状态。