Haematopoiesis and Leukocyte Biology Laboratory, Division of Immunometabolism, Baker Heart and Diabetes Institute, 75 Commercial Rd, 3004 Melbourne, Victoria, Australia.
Department of Immunology, Monash University, 89 Commercial Road, 3004 Melbourne, Victoria, Australia.
Eur Heart J. 2018 Jun 14;39(23):2158-2167. doi: 10.1093/eurheartj/ehy119.
Rheumatoid arthritis (RA) is associated with an approximately two-fold elevated risk of cardiovascular (CV)-related mortality. Patients with RA present with systemic inflammation including raised circulating myeloid cells, but fail to display traditional CV risk-factors, particularly dyslipidaemia. We aimed to explore if increased circulating myeloid cells is associated with impaired atherosclerotic lesion regression or altered progression in RA.
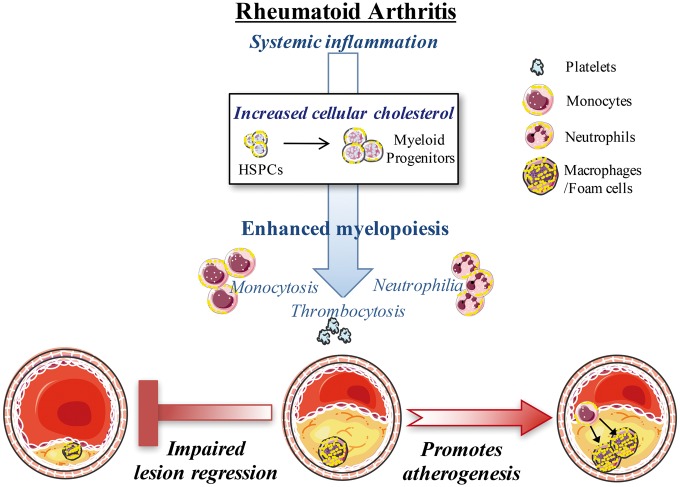
Using flow cytometry, we noted prominent monocytosis, neutrophilia, and thrombocytosis in two mouse models of RA. This was due to enhanced proliferation of the haematopoietic stem and progenitor cells (HSPCs) in the bone marrow and the spleen. HSPCs expansion was associated with an increase in the cholesterol content, due to a down-regulation of cholesterol efflux genes, Apoe, Abca1, and Abcg1. The HSPCs also had enhanced expression of key myeloid promoting growth factor receptors. Systemic inflammation was found to cause defective cellular cholesterol metabolism. Increased myeloid cells in mice with RA were associated with a significant impairment in lesion regression, even though cholesterol levels were equivalent to non-arthritic mice. Lesions from arthritic mice exhibited a less stable phenotype as demonstrated by increased immune cell infiltration, lipid accumulation, and decreased collagen formation. In a progression model, we noted monocytosis, enhanced monocytes recruitment to lesions, and increased plaque macrophages. This was reversed with administration of reconstituted high-density lipoprotein (rHDL). Furthermore, RA patients have expanded CD16+ monocyte subsets and a down-regulation of ABCA1 and ABCG1.
Rheumatoid arthritis impairs atherosclerotic regression and alters progression, which is associated with an expansion of myeloid cells and disturbed cellular cholesterol handling, independent of plasma cholesterol levels. Infusion of rHDL prevented enhanced myelopoiesis and monocyte entry into lesions. Targeting cellular cholesterol defects in people with RA, even if plasma cholesterol is within the normal range, may limit vascular disease.
类风湿关节炎(RA)与心血管(CV)相关死亡率升高约两倍相关。RA 患者表现出全身炎症,包括循环髓细胞升高,但不表现出传统的 CV 危险因素,特别是血脂异常。我们旨在探讨循环髓细胞增加是否与动脉粥样硬化病变消退受损或 RA 进展改变有关。
我们通过流式细胞术注意到两种 RA 小鼠模型中单核细胞增多症、中性粒细胞增多症和血小板增多症。这是由于骨髓和脾脏中的造血干细胞和祖细胞(HSPC)增殖增强所致。HSPC 扩增与胆固醇含量增加有关,这是由于胆固醇外排基因 Apoe、Abca1 和 Abcg1 的下调所致。HSPC 还具有关键髓系促进生长因子受体的增强表达。全身炎症被发现导致细胞胆固醇代谢缺陷。RA 小鼠中增加的髓细胞与病变消退显著受损有关,尽管胆固醇水平与非关节炎小鼠相当。关节炎小鼠的病变表现出更不稳定的表型,表现为免疫细胞浸润增加、脂质积累减少和胶原形成减少。在进展模型中,我们观察到单核细胞增多症、病变中单核细胞募集增强和斑块巨噬细胞增多。用重组高密度脂蛋白(rHDL)治疗可逆转这种情况。此外,RA 患者具有扩展的 CD16+单核细胞亚群和 ABCA1 和 ABCG1 的下调。
类风湿关节炎会损害动脉粥样硬化的消退并改变其进展,这与髓细胞的扩增和细胞胆固醇处理紊乱有关,与血浆胆固醇水平无关。rHDL 的输注可防止骨髓细胞过度生成和单核细胞进入病变。即使血浆胆固醇在正常范围内,靶向 RA 患者的细胞胆固醇缺陷也可能限制血管疾病的发生。