From the Departments of Neurology (S.H., T.T., P.v.W.-M., C.Z.S., N.H., A.T.M., T.H., M.S.P., N.R.d.M.A., D.D., G.A.) and Clinical Epidemiology (S.H., S.P.J., H.H.H.), Aarhus University Hospital; Department of Clinical Medicine, Aarhus University (S.H., C.Z.S., N.H., G.A); and Danish National Registers (H.H.H.), a National Quality Improvement Program (RKKP), Aarhus, Denmark.
Neurology. 2018 Jul 17;91(3):e236-e248. doi: 10.1212/WNL.0000000000005822. Epub 2018 Jun 15.
To investigate the effects of centralizing the acute stroke services in the Central Denmark Region (CDR).
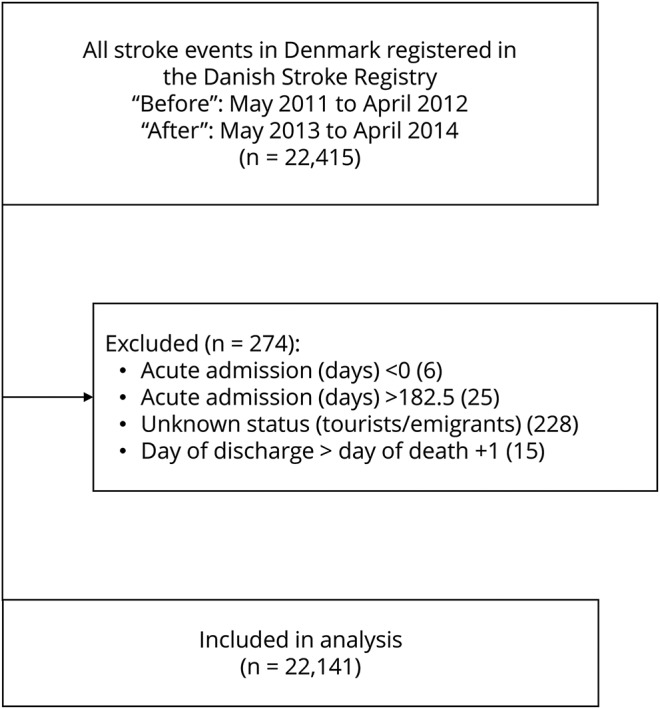
The CDR (1.3 million inhabitants) centralized acute stroke care from 6 to 2 designated acute stroke units with 7-day outpatient clinics. We performed a prospective "before-and-after" cohort study comparing all strokes from the CDR with strokes in the rest of Denmark to discover underlying general trends, adopting a difference-in-differences approach. The population comprised 22,141 stroke cases hospitalized from May 2011 to April 2012 and May 2013 to April 2014.
Centralization was associated with a significant reduction in length of acute hospital stay from a median of 5 to 2 days with a length-of-stay ratio of 0.53 (95% confidence interval 0.38-0.75, data adjusted) with no corresponding change seen in the rest of Denmark. Similarly, centralization led to a significant increase in strokes with same-day admission (mainly outpatients), whereas this remained unchanged in the rest of Denmark. We observed a significant improvement in quality of care captured in 11 process performance measures in both the CDR and the rest of Denmark. Centralization was associated with a nonsignificant increase in thrombolysis rate. We observed a slight increase in readmissions at day 30, but this was not significantly different from the general trend. Mortality at days 30 and 365 remained unchanged, as in the rest of Denmark.
Centralizing acute stroke care in the CDR significantly reduced the length of acute hospital stay without compromising quality. Readmissions and mortality stayed comparable to the rest of Denmark.
研究丹麦中部地区(CDR)集中急性脑卒中服务的效果。
CDR(130 万居民)将急性脑卒中护理从 6 家集中到 2 家指定的急性脑卒中单位,设有 7 天的门诊。我们进行了一项前瞻性“前后”队列研究,比较了 CDR 的所有脑卒中病例和丹麦其他地区的脑卒中病例,采用差异法发现潜在的总体趋势。该人群包括 2011 年 5 月至 2012 年 4 月和 2013 年 5 月至 2014 年 4 月住院的 22,141 例脑卒中病例。
集中化与急性住院时间的显著缩短相关,从中位数 5 天缩短至 2 天,住院时间比为 0.53(95%置信区间 0.38-0.75,数据调整),而丹麦其他地区没有相应变化。同样,集中化导致当天入院(主要为门诊患者)的脑卒中显著增加,而丹麦其他地区则保持不变。我们观察到在 CDR 和丹麦其他地区的 11 项流程绩效指标中,护理质量都得到了显著改善。集中化与溶栓率的非显著增加相关。我们观察到 30 天内再入院率略有增加,但与总体趋势无显著差异。30 天和 365 天的死亡率与丹麦其他地区保持不变。
CDR 集中急性脑卒中护理显著缩短了急性住院时间,而不影响护理质量。再入院率和死亡率与丹麦其他地区保持可比。