Pun Matiram, Hartmann Sara E, Furian Michael, Dyck Adrienna M, Muralt Lara, Lichtblau Mona, Bader Patrick R, Rawling Jean M, Ulrich Silvia, Bloch Konrad E, Poulin Marc J
Department of Physiology and Pharmacology, Cumming School of Medicine, University of Calgary, Calgary, AB, Canada.
Hotchkiss Brain Institute, Cumming School of Medicine, University of Calgary, Calgary, AB, Canada.
Front Physiol. 2018 Jun 4;9:677. doi: 10.3389/fphys.2018.00677. eCollection 2018.
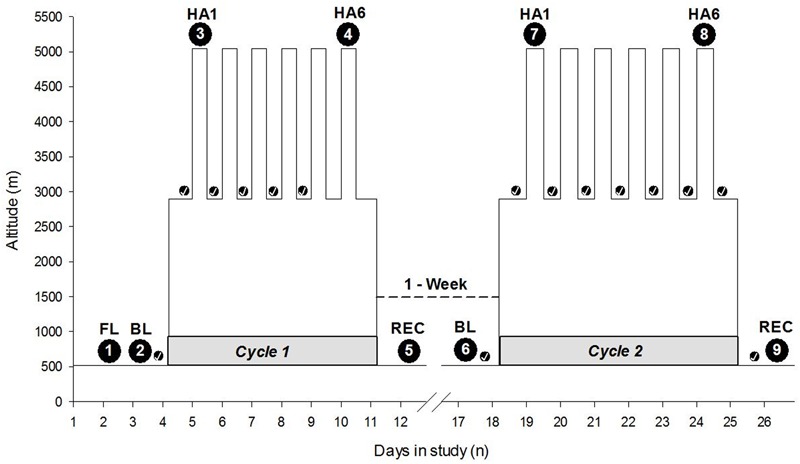
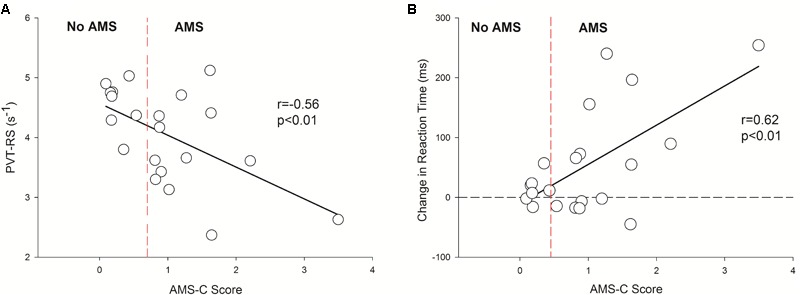
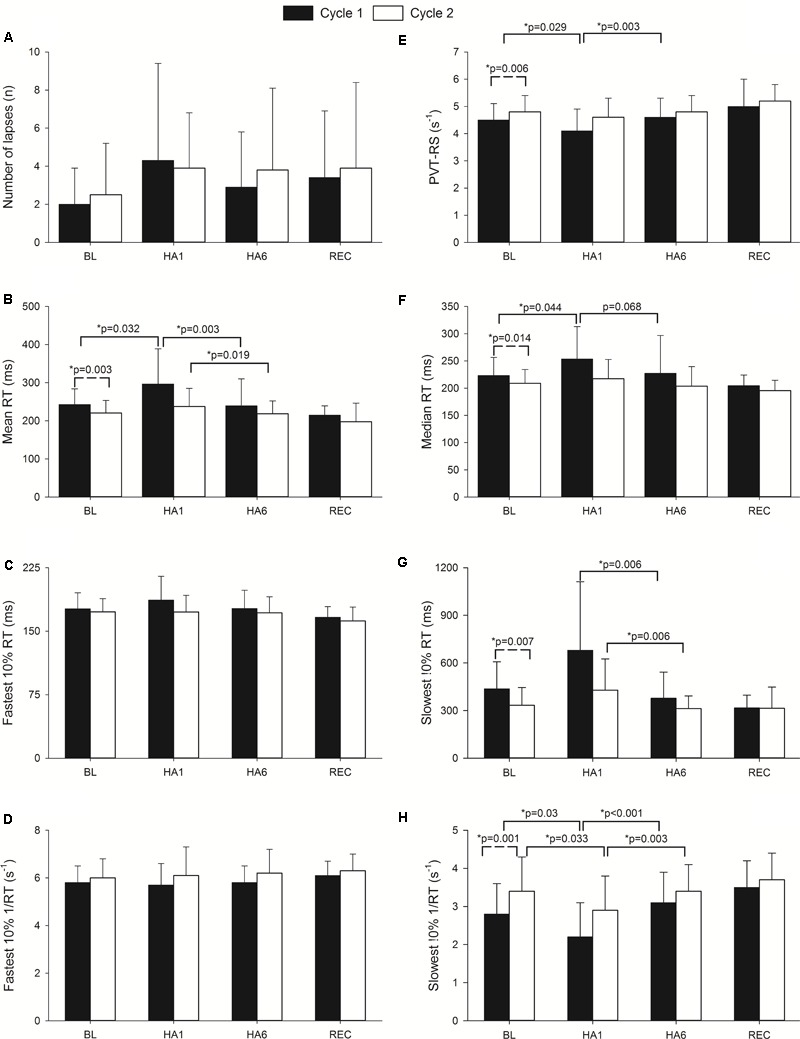
High altitude (HA) hypoxia may affect cognitive performance and sleep quality. Further, vigilance is reduced following sleep deprivation. We investigated the effect on vigilance, actigraphic sleep indices, and their relationships with acute mountain sickness (AMS) during very HA exposure, acclimatization, and re-exposure. A total of 21 healthy altitude-naive individuals (25 ± 4 years; 13 females) completed 2 cycles of altitude exposure separated by 7 days at low altitude (LA, 520 m). Participants slept at 2900 m and spent the day at HA, (5050 m). We report acute altitude exposure on Day 1 (LA vs. HA1) and after 6 days of acclimatization (HA1 vs. HA6). Vigilance was quantified by reaction speed in the 10-min psychomotor vigilance test reaction speed (PVT-RS). AMS was evaluated using the Environmental Symptoms Questionnaire Cerebral Score (AMS-C score). Nocturnal rest/activity was recorded to estimate sleep duration using actigraphy. In , PVT-RS was slower at HA1 compared to LA (4.1 ± 0.8 vs. 4.5 ± 0.6 s, respectively, = 0.029), but not at HA6 (4.6 ± 0.7; > 0.05). In , PVT-RS at HA1 (4.6 ± 0.7) and HA6 (4.8 ± 0.6) were not different from LA (4.8 ± 0.6, > 0.05) and significantly greater than corresponding values in . In both cycles, AMS scores were higher at HA1 than at LA and HA6 ( < 0.05). Estimated sleep durations (TST) at LA, 1st and 5th nights were 431.3 ± 28.7, 418.1 ± 48.6, and 379.7 ± 51.4 min, respectively, in and they were significantly reduced during acclimatization exposures (LA vs. 1st night, > 0.05; LA vs. 5th night, = 0.012; and 1st vs. 5th night, = 0.054). LA, 1st and 5th nights TST in were 477.5 ± 96.9, 430.9 ± 34, and 341.4 ± 32.2, respectively, and we observed similar deteriorations in TST as in (LA vs. 1st night, > 0.05; LA vs. 5th night, = 0.001; and 1st vs. 5th night, < 0.0001). At HA1, subjects who reported higher AMS-C scores exhibited slower PVT-RS ( = -0.56; < 0.01). Subjects with higher AMS-C scores took longer time to react to the stimuli during acute exposure ( = 0.62, < 0.01) during HA1 of . Acute exposure to HA reduces the PVT-RS. Altitude acclimatization over 6 days recovers the reaction speed and prevents impairments during subsequent altitude re-exposure after 1 week spent near sea level. However, acclimatization does not lead to improvement in total sleep time during acute and subacute exposures.
高海拔(HA)缺氧可能会影响认知能力和睡眠质量。此外,睡眠剥夺后警觉性会降低。我们研究了在极高海拔暴露、适应过程以及再次暴露期间,对警觉性、活动记录仪睡眠指标及其与急性高山病(AMS)之间关系的影响。共有21名从未去过高原的健康个体(25±4岁;13名女性)完成了2个周期的海拔暴露,中间间隔7天在低海拔(LA,520米)地区。参与者在2900米处睡眠,白天处于高海拔(5050米)环境。我们报告了第1天(LA与HA1)以及适应6天后(HA1与HA6)的急性海拔暴露情况。通过10分钟心理运动警觉性测试反应速度(PVT-RS)来量化警觉性。使用环境症状问卷脑部分数(AMS-C分数)评估AMS。通过活动记录仪记录夜间休息/活动情况以估计睡眠时间。在[第一个周期]中,与LA相比,HA1时的PVT-RS较慢(分别为4.1±0.8秒和4.5±0.6秒,P = 0.029),但HA6时并非如此(4.6±0.7;P>0.05)。在[第二个周期]中,HA1(4.6±0.7)和HA6(4.8±0.6)时的PVT-RS与LA(4.8±0.6)无差异(P>0.05),且显著高于[第一个周期]中的相应值。在两个周期中,HA1时的AMS分数均高于LA和HA6时(P<0.05)。在[第一个周期]中,LA、第1晚和第5晚的估计睡眠时间(TST)分别为431.3±28.7、418.1±48.6和379.7±51.4分钟,在适应暴露期间睡眠时间显著减少(LA与第1晚比较,P>0.05;LA与第5晚比较,P = 0.012;第1晚与第5晚比较,P = 0.054)。在[第二个周期]中,LA、第1晚和第5晚的TST分别为477.5±96.9、430.9±34和341.4±32.2分钟,我们观察到TST的恶化情况与[第一个周期]类似(LA与第1晚比较,P>0.05;LA与第5晚比较,P = 0.001;第1晚与第5晚比较,P<0.0001)。在HA1时,报告AMS-C分数较高的受试者PVT-RS较慢(r = -0.56;P<0.01)。在[第一个周期]的HA1期间,AMS-C分数较高的受试者对刺激的反应时间更长(r = 0.62,P<0.01)。急性暴露于HA会降低PVT-RS。经过6天的海拔适应可恢复反应速度,并防止在海平面附近度过1周后再次进行海拔暴露时出现损伤。然而,适应并不会导致急性和亚急性暴露期间总睡眠时间的改善。