Lopez Segui Francesc, Pratdepadua Bufill Carme, Abdon Gimenez Nuria, Martinez Roldan Jordi, Garcia Cuyas Francesc
TIC Salut Social, Generalitat de Catalunya, Mataró, Barcelona, Spain.
Centre for Research in Health and Economics, Department of Experimental and Health Sciences, Universitat Pompeu Fabra, Barcelona, Spain.
JMIR Mhealth Uhealth. 2018 Jun 21;6(6):e10701. doi: 10.2196/10701.
In Catalonia, the Fundació TIC Salut Social's mHealth Office created the AppSalut Site to showcase to mobile apps in the field of health and social services. Its primary objective was to encourage the public to look after their health. The catalogue allows primary health care doctors to prescribe certified, connected apps, which guarantees a safe and reliable environment for their use. The generated data can be consulted by health care professionals and included in the patient's clinical history. This document presents the intervention and the major findings following a five-month pilot project conducted in the Barcelona area.
The objective of the pilot study was to test, in a real, controlled environment, the implementation of AppSalut. Specifically, we tested whether (1) the procedures corresponding to the prescription, transmission, and evaluation of the data functions correctly, (2) users interact successfully and accept the tool, and (3) the data travels through existing pathways in accordance with international standards. The evaluation is not based on clinical criteria, but rather on the usability and technological reliability of the intervention and its implementation in the context of primary care.
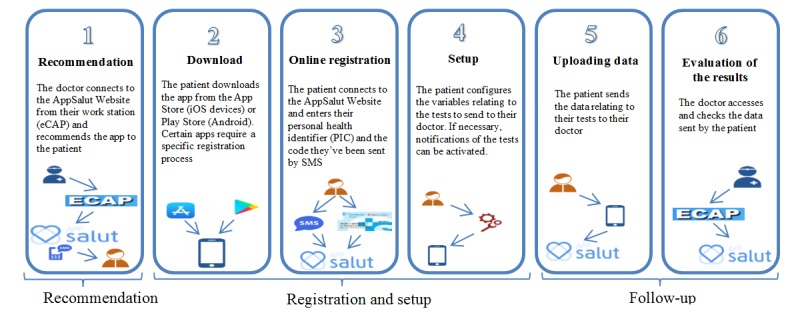
The project was presented to the Primary Care Team participants to encourage the involvement of doctors. The study involved at least 5 doctors and 5 patients per professional, chosen at their discretion and in accordance with their own clinical criteria. An initial consultation took place, during which the doctor discussed the pilot project with the patient and recommended the app. The patient was sent a text message (SMS, short message service) containing an access code. When the patient arrived home, they accessed their personal health record (PHR) to view the recommendation, download the app, and enter the access code. The patient was then able to start using the app. The data was collected in a standardized manner and automatically sent to the system. In a second visit, the patient looked at the data with their doctor on their clinical station screen. The latter was able to consult the information generated by the patient and select what to include in their electronic health record. In order to assess the performance of the system, three focus groups were performed and two ad-hoc case-specific questionnaires, one for doctors and one for patients, were sent by email. Response was voluntary.
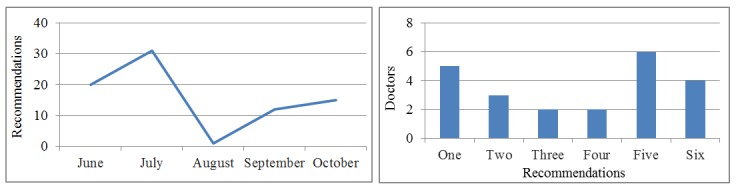
A total of 32 doctors made 79 recommendations of apps to patients. On average, the patients uploaded data 13 times per prescribed app, accounting for a total of 16 different variables. Results show that data traveled through the established channels in an adequate manner and in accordance with international standards. This includes the prescription of an app by a doctor, the patient accessing the recommendation via the PHR, app download by the patient from the official app stores, linking of the patient to the public platform through the app, the generation and visualization of the data on the primary care workstation, and its subsequent validation by the clinician.
First, the choice of apps to be used is fundamental; the user's perception of the utility of the proposed tool being paramount. Second, thorough face-to-face support is vital for a smooth transition towards a more intense model of telemedicine. Last, a powerful limiting factor is the lack of control over people's ability to use the apps.
在加泰罗尼亚,“健康与社会服务技术创新基金会”的移动健康办公室创建了“健康应用平台”,用于展示健康和社会服务领域的移动应用程序。其主要目标是鼓励公众关注自身健康。该目录允许初级保健医生开具经过认证的联网应用程序,从而确保使用环境的安全可靠。医疗保健专业人员可以查阅生成的数据,并将其纳入患者的临床病史。本文介绍了在巴塞罗那地区进行的为期五个月的试点项目的干预措施和主要发现。
试点研究的目的是在真实、可控的环境中测试“健康应用平台”的实施情况。具体而言,我们测试了以下内容:(1)与数据功能的开具、传输和评估相关的程序是否正确运行;(2)用户是否能够成功交互并接受该工具;(3)数据是否按照国际标准通过现有途径传输。评估并非基于临床标准,而是基于干预措施的可用性和技术可靠性及其在初级保健背景下的实施情况。
该项目向初级保健团队参与者进行了介绍,以鼓励医生参与。该研究要求每位专业人员至少选择5名医生和5名患者,由他们自行决定并根据自己的临床标准进行选择。进行了初步咨询,在此期间医生与患者讨论了试点项目并推荐了应用程序。向患者发送了一条包含访问代码的短信。患者到家后,他们访问个人健康记录(PHR)以查看推荐内容、下载应用程序并输入访问代码。然后患者就可以开始使用该应用程序。数据以标准化方式收集并自动发送到系统。在第二次就诊时,患者与医生在临床工作站屏幕上查看数据。医生能够查阅患者生成的信息,并选择将哪些信息纳入其电子健康记录。为了评估系统的性能,进行了三个焦点小组讨论,并通过电子邮件发送了两份针对特定案例的临时问卷,一份给医生,一份给患者。回复是自愿的。
共有32名医生向患者推荐了79款应用程序。平均而言,患者为每个开具的应用程序上传数据13次,总共涉及16个不同变量。结果表明,数据以适当的方式并按照国际标准通过既定渠道传输。这包括医生开具应用程序、患者通过PHR访问推荐内容、患者从官方应用商店下载应用程序、患者通过应用程序链接到公共平台、在初级保健工作站上生成和查看数据以及随后由临床医生进行验证。
首先,选择要使用的应用程序至关重要;用户对所提议工具实用性的认知最为关键。其次,全面的面对面支持对于顺利过渡到更强化的远程医疗模式至关重要。最后,一个强大的限制因素是对人们使用应用程序能力的控制不足。