Department of General Practice & Elderly Care, University Medical Center Groningen, Groningen Research Institute for Asthma and COPD (GRIAC), University of Groningen, Groningen, The Netherlands.
Department of Pharmacy, Unit of Pharmacoepidemiology & Pharmacoeconomics, University of Groningen, Groningen, The Netherlands.
NPJ Prim Care Respir Med. 2018 Jun 27;28(1):24. doi: 10.1038/s41533-018-0092-8.
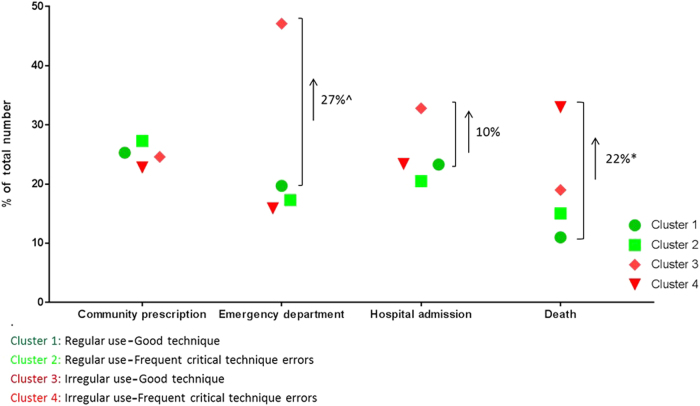
Four inhaler adherence clusters have been identified using the INCA audio device in COPD patients: (1) regular use/good technique, (2) regular use/frequent technique errors, (3) irregular use/good technique, and (4) irregular use/frequent technique errors. Their relationship with healthcare utilization and mortality was established, but the cost-effectiveness of adherence-enhancing interventions is unknown. In this exploratory study, we aimed to estimate the potential cost-effectiveness of reaching optimal adherence in the three suboptimal adherence clusters, i.e., a theoretical shift of clusters 2, 3, and 4 to cluster 1. Cost-effectiveness was estimated over a 5-year time horizon using the Irish healthcare payer perspective. We used a previously developed COPD health-economic model that was updated with INCA trial data and Irish national economic and epidemiological data. For each cluster, interventions would result in additional quality-adjusted life years gained at reasonable investment. Cost-effectiveness was most favorable in cluster 3, with possible cost savings of €845/annum/person.
已经使用 INCA 音频设备在 COPD 患者中确定了四个吸入器依从性集群:(1)常规使用/良好技术,(2)常规使用/频繁技术错误,(3)不规则使用/良好技术,和(4)不规则使用/频繁技术错误。已经确定了它们与医疗保健利用和死亡率的关系,但尚不清楚增强依从性干预的成本效益。在这项探索性研究中,我们旨在估计在三个次优依从性集群中达到最佳依从性的潜在成本效益,即集群 2、3 和 4 的理论转变为集群 1。使用爱尔兰医疗保健支付者的观点,在 5 年的时间内估算成本效益。我们使用了先前开发的 COPD 健康经济学模型,该模型使用 INCA 试验数据和爱尔兰国家经济和流行病学数据进行了更新。对于每个集群,干预措施将在合理投资的情况下带来额外的质量调整生命年获益。在集群 3 中成本效益最为有利,可能每年每人节省 845 欧元。