Department of Health Services Research, CAPHRI, Maastricht University, P.O. Box 616, 6200, Maastricht, The Netherlands.
Son Pisa Primary Health Care Centre, Balearic Health Service, Palma de Mallorca, Spain.
NPJ Prim Care Respir Med. 2017 Apr 13;27(1):24. doi: 10.1038/s41533-017-0022-1.
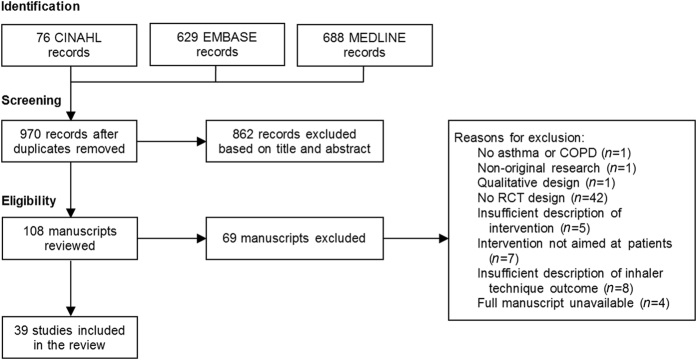
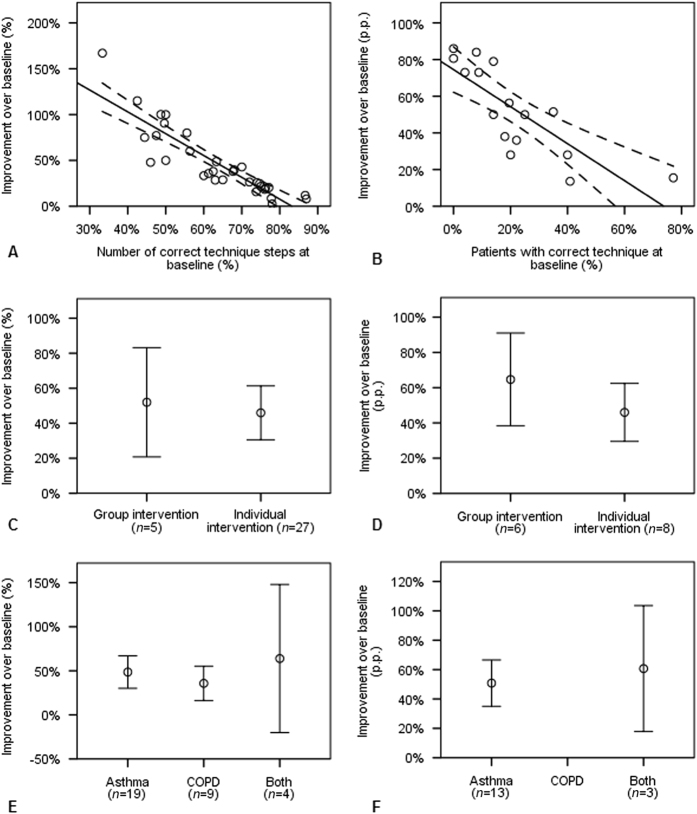
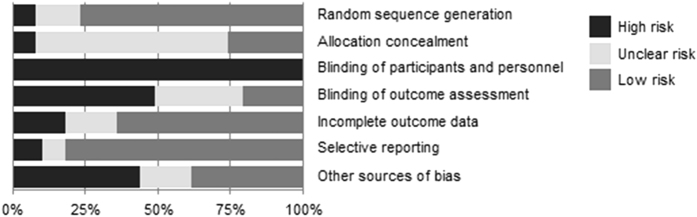
With the current wealth of new inhalers available and insurance policy driven inhaler switching, the need for insights in optimal education on inhaler use is more evident than ever. We aimed to systematically review educational inhalation technique interventions, to assess their overall effectiveness, and identify main drivers of success. Medline, Embase and CINAHL databases were searched for randomised controlled trials on educational inhalation technique interventions. Inclusion eligibility, quality appraisal (Cochrane's risk of bias tool) and data extraction were performed by two independent reviewers. Regression analyses were performed to identify characteristics contributing to inhaler technique improvement. Thirty-seven of the 39 interventions included (95%) indicated statistically significant improvement of inhaler technique. However, average follow-up time was relatively short (5 months), 28% lacked clinical relevant endpoints and all lacked cost-effectiveness estimates. Poor initial technique, number of inhalation procedure steps, setting (outpatient clinics performing best), and time elapsed since intervention (all, p < 0.05), were shown to have an impact on effectiveness of the intervention, explaining up to 91% of the effectiveness variation. Other factors, such as disease (asthma vs. chronic obstructive pulmonary disease), education group size (individual vs. group training) and inhaler type (dry powder inhalers vs. pressurised metered dose inhalers) did not play a significant role. Notably, there was a trend (p = 0.06) towards interventions in adults being more effective than those in children and the intervention effect seemed to wane over time. In conclusion, educational interventions to improve inhaler technique are effective on the short-term. Periodical intervention reinforcement and longer follow-up studies, including clinical relevant endpoints and cost-effectiveness, are recommended.
随着目前新型吸入器的大量出现以及保险政策驱动的吸入器更换,对吸入器使用进行最佳教育的需求比以往任何时候都更加明显。我们旨在系统地回顾教育吸入技术干预措施,评估其总体效果,并确定成功的主要驱动因素。我们在 Medline、Embase 和 CINAHL 数据库中搜索了关于教育吸入技术干预措施的随机对照试验。纳入标准、质量评估(Cochrane 偏倚风险工具)和数据提取由两名独立审查员进行。进行回归分析以确定有助于吸入器技术改进的特征。39 项干预措施中有 37 项(95%)表明吸入器技术有统计学上的显著改善。然而,平均随访时间相对较短(5 个月),28%的研究缺乏临床相关终点,所有研究都缺乏成本效益评估。初始技术差、吸入步骤数量、环境(门诊诊所效果最佳)以及干预后时间(均,p<0.05),都对干预效果产生影响,可解释高达 91%的效果变异。其他因素,如疾病(哮喘与慢性阻塞性肺疾病)、教育组规模(个体与小组培训)和吸入器类型(干粉吸入器与压力定量吸入器),则没有起到显著作用。值得注意的是,成人干预比儿童干预更有效(p=0.06),且干预效果似乎随时间推移而减弱。总之,教育干预措施可在短期内有效改善吸入器技术。建议定期进行干预强化,并开展更长时间的随访研究,包括临床相关终点和成本效益。