Sawhney Simon, Robinson Heather A, van der Veer Sabine N, Hounkpatin Hilda O, Scale Timothy M, Chess James A, Peek Niels, Marks Angharad, Davies Gareth Ivor, Fraccaro Paolo, Johnson Matthew J, Lyons Ronan A, Nitsch Dorothea, Roderick Paul J, Halbesma Nynke, Miller-Hodges Eve, Black Corrinda, Fraser Simon
Institute of Applied Health Sciences, University of Aberdeen, Aberdeen, UK.
Farr Institute of Health Informatics Research, UK.
BMJ Open. 2018 Jun 30;8(6):e019435. doi: 10.1136/bmjopen-2017-019435.
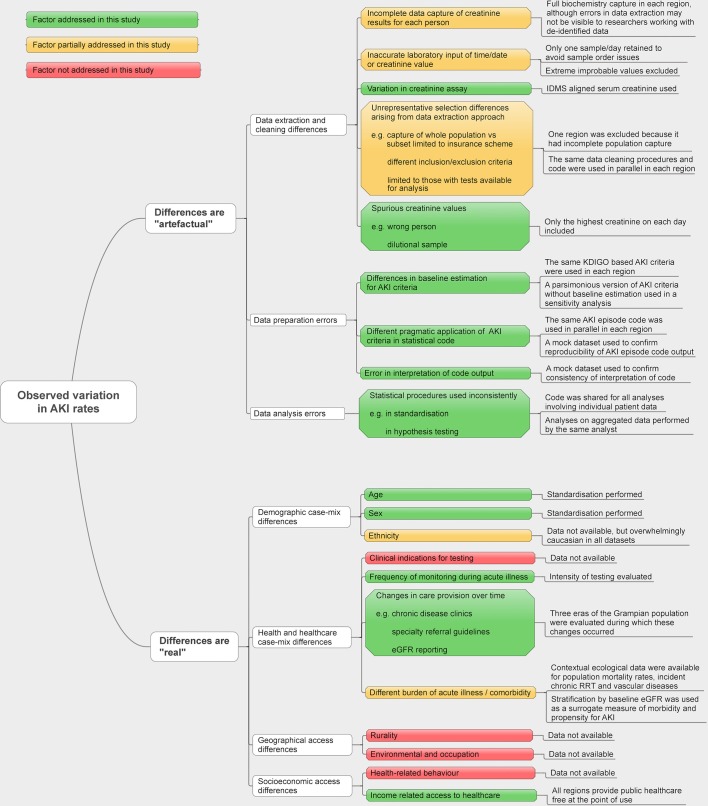
A rapid growth in the reported rates of acute kidney injury (AKI) has led to calls for greater attention and greater resources for improving care. However, the reported incidence of AKI also varies more than tenfold between previous studies. Some of this variation is likely to stem from methodological heterogeneity. This study explores the extent of cross-population variation in AKI incidence after minimising heterogeneity.
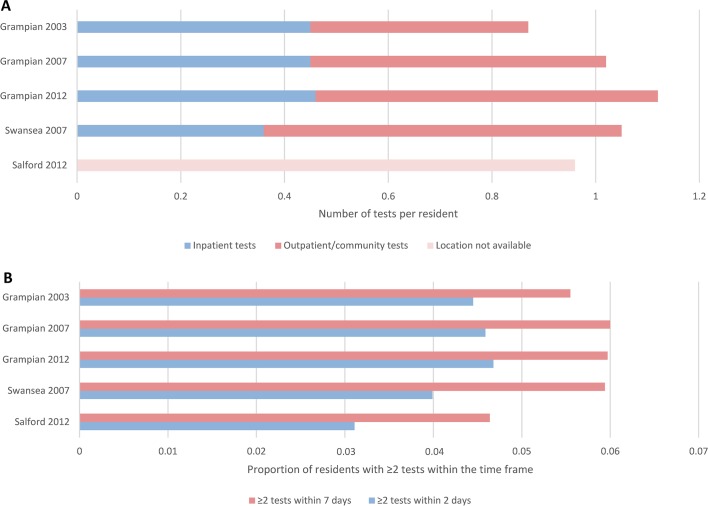
Population-based cohort study analysing data from electronic health records from three regions in the UK through shared analysis code and harmonised methodology.
Three populations from Scotland, Wales and England covering three time periods: Grampian 2003, 2007 and 2012; Swansea 2007; and Salford 2012.
All residents in each region, aged 15 years or older.
Population incidence of AKI and AKI phenotype (severity, recovery, recurrence). Determined using shared biochemistry-based AKI episode code and standardised by age and sex.
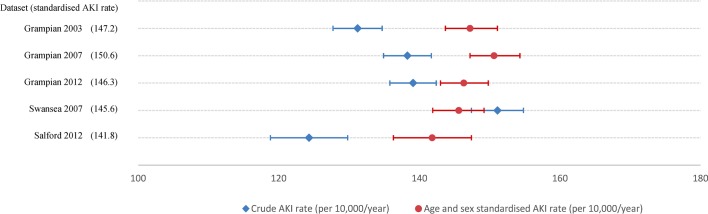
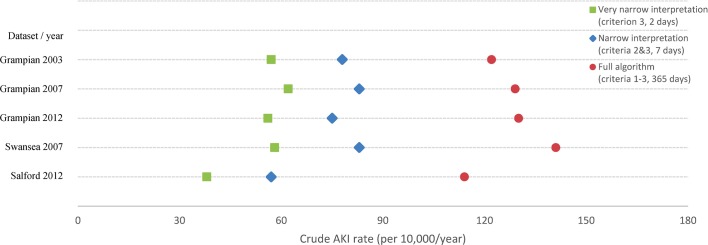
Respectively, crude AKI rates (per 10 000/year) were 131, 138, 139, 151 and 124 (p=0.095), and after standardisation for age and sex: 147, 151, 146, 146 and 142 (p=0.257) for Grampian 2003, 2007 and 2012; Swansea 2007; and Salford 2012. The pattern of variation in crude rates was robust to any modifications of the AKI definition. Across all populations and time periods, AKI rates increased substantially with age from ~20 to ~550 per 10 000/year among those aged <40 and ≥70 years.
When harmonised methods are used and age and sex differences are accounted for, a similar high burden of AKI is consistently observed across different populations and time periods (~150 per 10 000/year). There are particularly high rates of AKI among older people. Policy-makers should be careful not draw simplistic assumptions about variation in AKI rates based on comparisons that are not rigorous in methodological terms.
急性肾损伤(AKI)报告发病率的快速增长促使人们呼吁给予更多关注并投入更多资源来改善治疗。然而,先前研究中报告的AKI发病率差异超过十倍。这种差异部分可能源于方法学的异质性。本研究旨在探讨在最小化异质性后,不同人群中AKI发病率的差异程度。
基于人群的队列研究,通过共享分析代码和统一方法分析来自英国三个地区电子健康记录的数据。
来自苏格兰、威尔士和英格兰的三个人群,涵盖三个时间段:格兰扁地区2003年、2007年和2012年;斯旺西2007年;索尔福德2012年。
每个地区15岁及以上的所有居民。
AKI的人群发病率及AKI表型(严重程度、恢复情况、复发情况)。使用基于共享生物化学的AKI发作代码确定,并按年龄和性别进行标准化。
格兰扁地区2003年、2007年和2012年、斯旺西2007年、索尔福德2012年的AKI粗发病率(每10000人/年)分别为131、138、139、151和124(p = 0.095),经年龄和性别标准化后分别为147、151、146、146和142(p = 0.257)。粗发病率的变化模式对AKI定义的任何修改均具有稳健性。在所有人群和时间段中,AKI发病率随年龄大幅增加,年龄<40岁和≥70岁人群中从约每10000人/年20增至约550。
当采用统一方法并考虑年龄和性别差异时,在不同人群和时间段中始终观察到类似的高AKI负担(约每10000人/年150)。老年人中的AKI发病率尤其高。政策制定者应谨慎,不要基于方法学上不严谨的比较对AKI发病率的差异做出简单假设。