Haj Magda, Haj Mona, Rockey Don C
American University of Beirut Medical Center, Beirut, Lebanon Department of Internal Medicine and the Division of Gastroenterology and Hepatology, Medical University of South Carolina, Charleston, SC.
Medicine (Baltimore). 2018 Jul;97(27):e11187. doi: 10.1097/MD.0000000000011187.
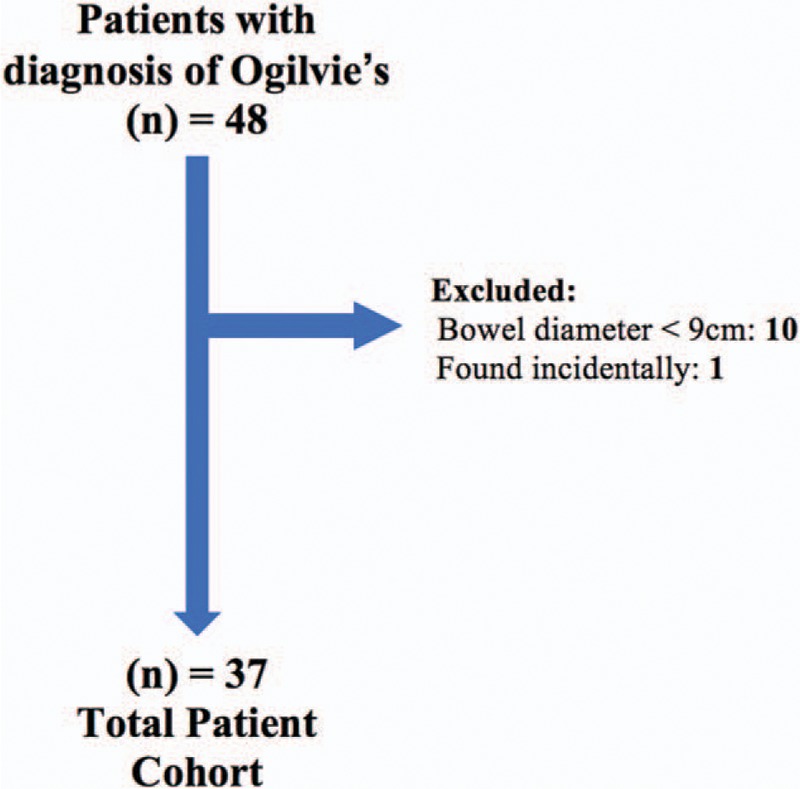
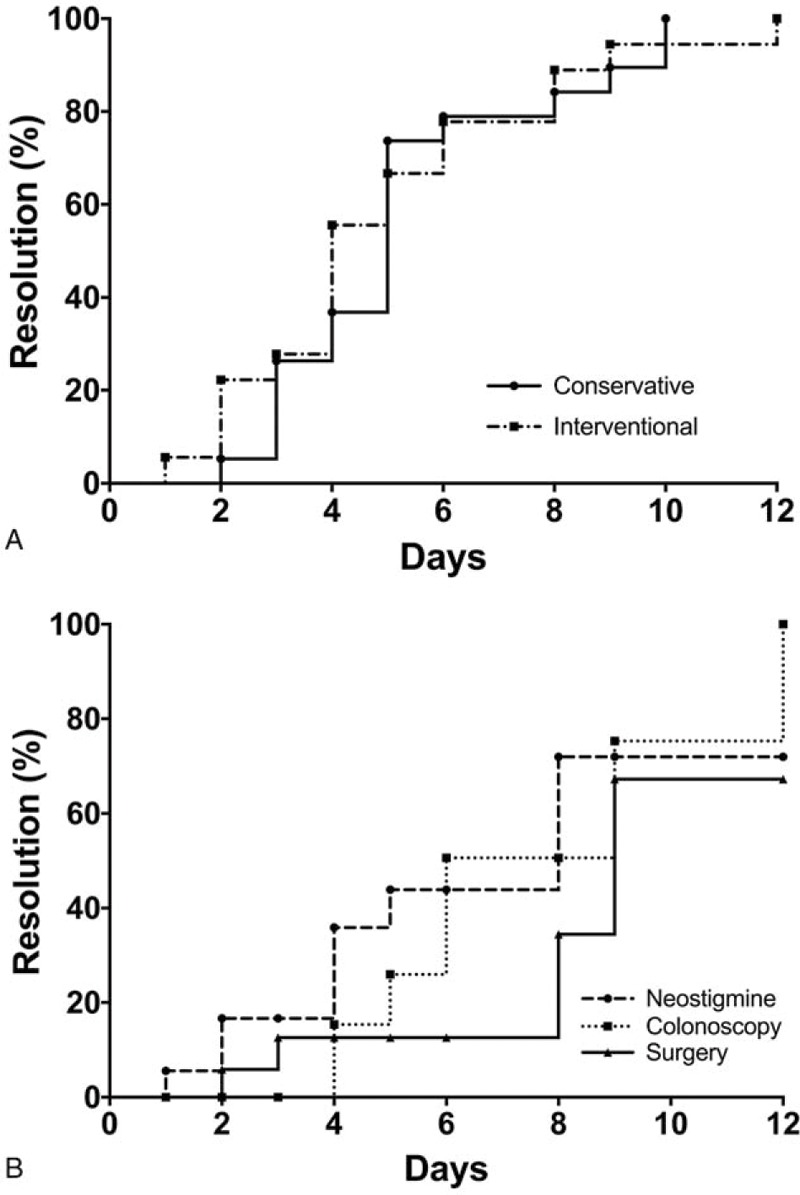
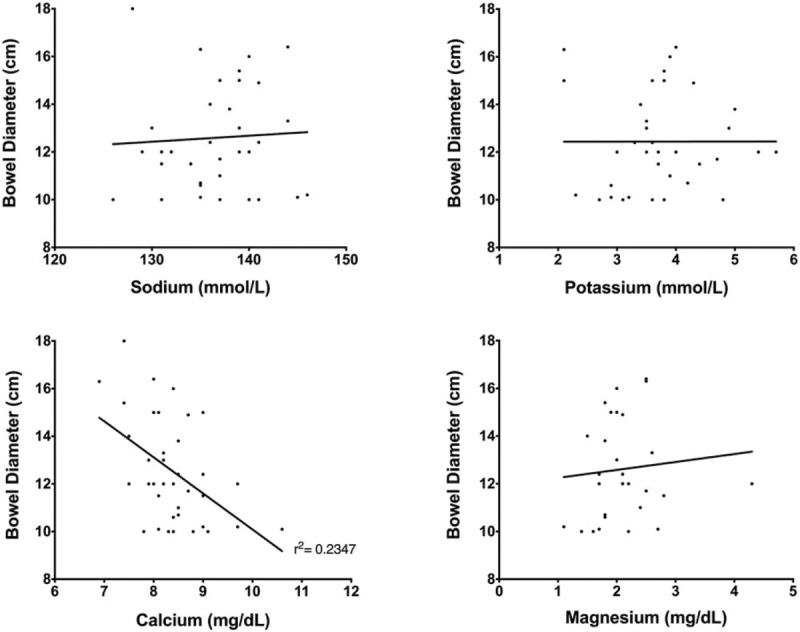
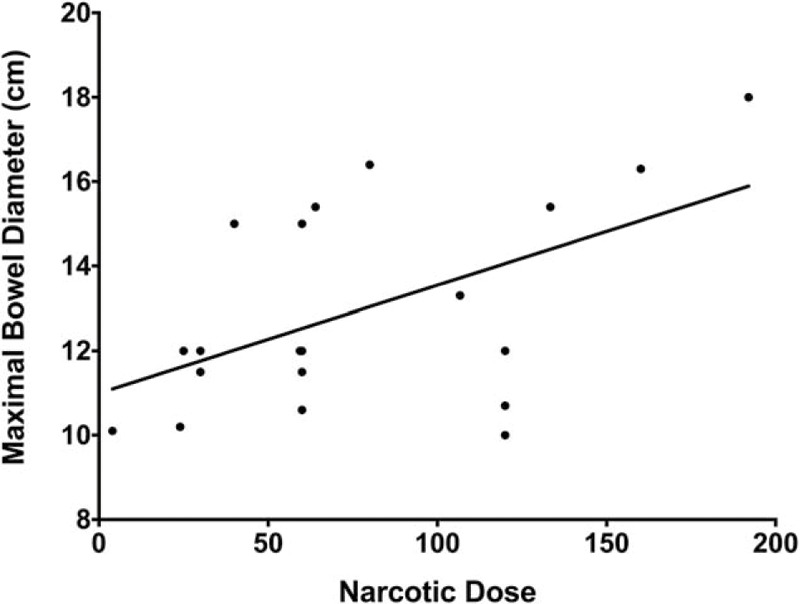
Ogilvie's syndrome, also known as acute colonic pseudo-obstruction, refers to pathologic dilation of the colon without underlying mechanical obstruction, occurring primarily in patients with serious comorbidities. Diagnosis of Ogilvie's syndrome is based on clinical and radiologic grounds, and can be treated conservatively or with interventions such as acetylcholinesterase inhibitors (such as neostigmine), decompressive procedures including colonoscopy, and even surgery. Based on our clinical experience we hypothesized that conservative management yields similar, if not superior, results to interventional management. Therefore, we retrospectively examined all patients over the age of 18 with Ogilvie's syndrome who presented to the Medical University of South Carolina (MUSC). The diagnosis of Ogilvie's syndrome was confirmed by clinical criteria, including imaging evidence of colonic dilation ≥9 cm. Patients were divided and analyzed in 2 groups based on management: conservative (observation, rectal tube, nasogastric tube, fluid resuscitation, and correction of electrolytes) and interventional (neostigmine, colonoscopy, and surgery). Use of narcotics in relation to maximal bowel size was also analyzed. Over the 11-year study period (2005-2015), 37 patients with Ogilvie's syndrome were identified. The average age was 67 years and the average maximal bowel diameter was 12.5 cm. Overall, 19 patients (51%) were managed conservatively and 18 (49%) underwent interventional management. There was no significant difference in bowel dilation (12.0 cm vs 13.0 cm; P = .21), comorbidities (based on the Charlson Comorbidity Index (CCI), 3.2 vs 3.4; P = .74), or narcotic use (P = .79) between the conservative and interventional management groups, respectively. Of the 18 patients undergoing interventional management, 11 (61%) had Ogilvie's-syndrome-related complications compared to 4 (21%) of the 19 patients in the conservative management group (P < .01). There was no difference in overall length of stay in the 2 groups. Two patients, one in each group, died from complications unrelated to their Ogilvie's syndrome. We conclude that Ogilvie's syndrome, although uncommon, and typically associated with severe underlying disease, is currently associated with a low inpatient mortality. While interventional management is often alluded to in the literature, we found no evidence that aggressive measures lead to improved outcomes.
奥吉尔维综合征,又称急性结肠假性梗阻,是指结肠病理性扩张但无潜在机械性梗阻,主要发生在患有严重合并症的患者中。奥吉尔维综合征的诊断基于临床和影像学依据,可采用保守治疗或使用诸如乙酰胆碱酯酶抑制剂(如新斯的明)、包括结肠镜检查在内的减压措施甚至手术等干预手段进行治疗。根据我们的临床经验,我们推测保守治疗即使不比干预治疗效果更好,也会产生相似的结果。因此,我们回顾性研究了所有18岁以上患有奥吉尔维综合征并就诊于南卡罗来纳医科大学(MUSC)的患者。奥吉尔维综合征的诊断通过临床标准得到证实,包括结肠扩张≥9厘米的影像学证据。根据治疗方法将患者分为两组进行分析:保守治疗组(观察、直肠管、鼻胃管、液体复苏和电解质纠正)和干预治疗组(新斯的明、结肠镜检查和手术)。还分析了与最大肠径相关的麻醉药物使用情况。在11年的研究期间(2005 - 2015年),共确定了37例奥吉尔维综合征患者。平均年龄为67岁,平均最大肠径为12.5厘米。总体而言,19例患者(51%)接受了保守治疗,18例(49%)接受了干预治疗。保守治疗组和干预治疗组在肠扩张(12.0厘米对13.0厘米;P = 0.21)、合并症(基于查尔森合并症指数(CCI),3.2对3.4;P = 0.74)或麻醉药物使用(P = 0.79)方面分别无显著差异。在接受干预治疗的18例患者中,11例(61%)出现了与奥吉尔维综合征相关的并发症,而保守治疗组的19例患者中有4例(21%)出现相关并发症(P < 0.01)。两组的总住院时间无差异。两组各有1例患者死于与奥吉尔维综合征无关的并发症。我们得出结论,奥吉尔维综合征虽然不常见,且通常与严重的基础疾病相关,但目前住院死亡率较低。虽然文献中经常提到干预治疗,但我们没有发现积极措施能改善预后的证据。