Wang Meijiao, Li Sha, Huang Yuliang, Yue Haizhen, Li Tian, Wu Hao, Gao Song, Zhang Yibao
Key Laboratory of Carcinogenesis and Translational Research (Ministry of Education/Beijing), Department of Radiation Oncology, Beijing Cancer Hospital & Institute, Peking University Cancer Hospital & Institute, Beijing, China.
Department of Medical Physics, Institute of Medical Humanities, Peking University, Beijing, China.
J Appl Clin Med Phys. 2018 Sep;19(5):491-498. doi: 10.1002/acm2.12403. Epub 2018 Jul 8.
To test if a RapidPlan DVH estimation model and its training plans can be improved interactively through a closed-loop evolution process.
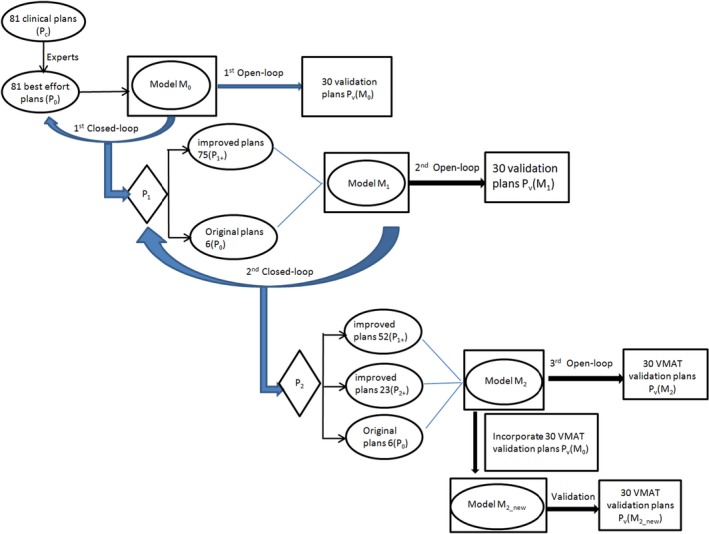
Eighty-one manual plans (P ) that were used to configure an initial rectal RapidPlan model (M ) were reoptimized using M (closed-loop), yielding 81 P plans. The 75 improved P (P ) and the remaining 6 P were used to configure model M . The 81 training plans were reoptimized again using M , producing 23 P plans that were superior to both their P and P forms (P ). Hence, the knowledge base of model M composed of 6 P , 52 P , and 23 P . Models were tested dosimetrically on 30 VMAT validation cases (P ) that were not used for training, yielding P (M ), P (M ), and P (M ) respectively. The 30 P were also optimized by M as trained by the library of M and 30 P (M ).
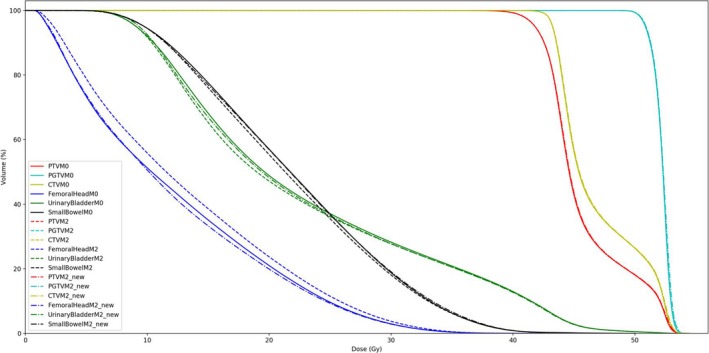
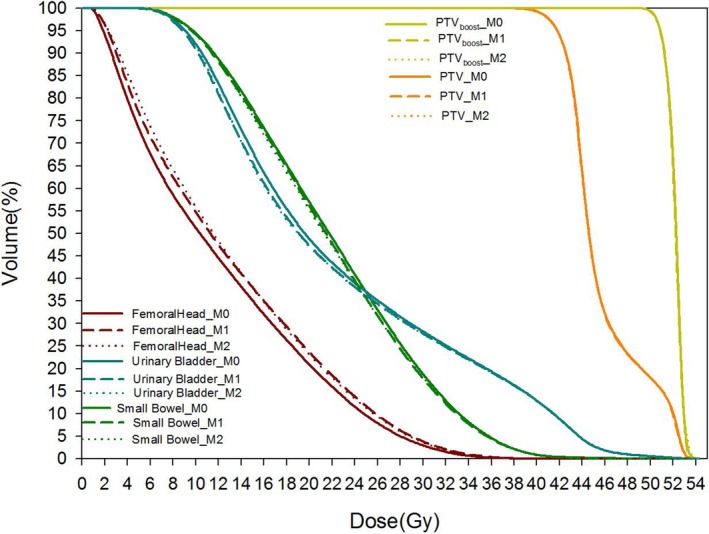
Based on comparable target dose coverage, the first closed-loop reoptimization significantly (P < 0.01) reduced the 81 training plans' mean dose to femoral head, urinary bladder, and small bowel by 2.65 Gy/15.63%, 2.06 Gy/8.11%, and 1.47 Gy/6.31% respectively, which were further reduced significantly (P < 0.01) in the second closed-loop reoptimization by 0.04 Gy/0.28%, 0.18 Gy/0.77%, 0.22 Gy/1.01% respectively. However, open-loop VMAT validations displayed more complex and intertwined plan quality changes: mean dose to urinary bladder and small bowel decreased monotonically using M (by 0.34 Gy/1.47%, 0.25 Gy/1.13%) and M (by 0.36 Gy/1.56%, 0.30 Gy/1.36%) than using M . However, mean dose to femoral head increased by 0.81 Gy/6.64% (M ) and 0.91 Gy/7.46% (M ) than using M . The overfitting problem was relieved by applying model M .
The RapidPlan model and its constituent plans can improve each other interactively through a closed-loop evolution process. Incorporating new patients into the original training library can improve the RapidPlan model and the upcoming plans interactively.
测试快速计划剂量体积直方图(DVH)估计模型及其训练计划能否通过闭环演化过程进行交互式改进。
用于配置初始直肠快速计划模型(M)的81个手动计划(P)使用M进行重新优化(闭环),得到81个P计划。75个改进后的P(P)和其余6个P用于配置模型M。使用M再次对81个训练计划进行重新优化,产生23个优于其P和P形式的P计划(P)。因此,模型M的知识库由6个P、52个P和23个P组成。在30个未用于训练的容积调强放疗(VMAT)验证病例(P)上对模型进行剂量学测试,分别得到P(M)、P(M)和P(M)。30个P也由M按照M库训练的方式进行优化,得到30个P(M)。
基于可比的靶区剂量覆盖,第一次闭环重新优化显著(P < 0.01)降低了81个训练计划对股骨头、膀胱和小肠 的平均剂量,分别降低了2.65 Gy/15.63%、2.06 Gy/8.11%和1.47 Gy/6.31%,在第二次闭环重新优化中进一步显著(P < 0.01)降低,分别为0.04 Gy/0.28%、0.18 Gy/0.77%、0.22 Gy/1.01%。然而,开环VMAT验证显示出更复杂且相互交织的计划质量变化情况:使用M(分别降低0.34 Gy/1.47%、0.25 Gy/1.13%)和M(分别降低0.36 Gy/1.56%、0.30 Gy/1.36%)时,膀胱和小肠的平均剂量比使用M时单调下降。然而,使用M时,股骨头的平均剂量比使用M时分别增加了0.81 Gy/6.64%(M)和0.91 Gy/7.46%(M)。应用模型M缓解了过拟合问题。
快速计划模型及其组成计划可通过闭环演化过程进行交互式改进。将新患者纳入原始训练库可交互式改进快速计划模型和后续计划。