Chen Kenneth, Tay Kae Jack, Law Yan Mee, Aydin Hakan, Ho Henry, Cheng Christopher, Yuen John Shyi Peng
Department of Urology, Singapore General Hospital, Singapore.
Department of Diagnostic Radiology, Singapore General Hospital, Singapore.
Asian J Urol. 2018 Jul;5(3):184-193. doi: 10.1016/j.ajur.2017.07.001. Epub 2017 Jul 12.
Active surveillance (AS) offers a strategy to reduce overtreatment and now is a widely accepted treatment option for low-risk prostate cancer. An ideal tool for risk-stratification would detect aggressive cancers and exclude such men from taking up AS in the first place. We evaluate if a combination of transperineal template biopsy with magnetic resonance imaging (MRI)-targeted biopsy identifies significant prostate cancer amongst men initially diagnosed with low-risk prostate cancer.
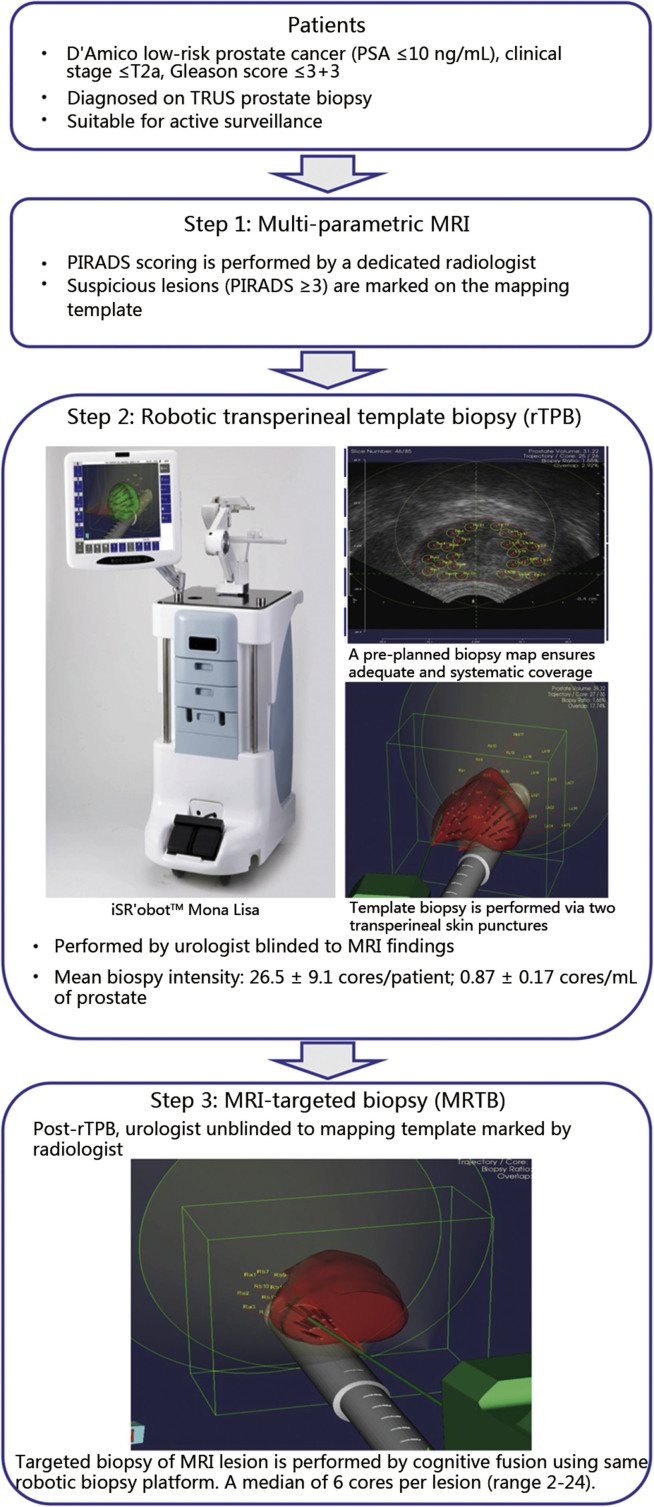
This prospective, single-blinded study included men with low-risk prostate cancer (D'Amico's Criteria) diagnosed on conventional transrectal ultrasound-guided biopsy. Patients first underwent multiparametric MRI of the prostate ≥6 weeks after initial biopsy. Each suspicious lesion is mapped and assigned a Prostate Imaging Reporting and Data System (PIRADS) score. Template biopsy is first performed with the surgeon blinded to MRI findings followed by MRI-targeted biopsy using a robotic transperineal biopsy platform.
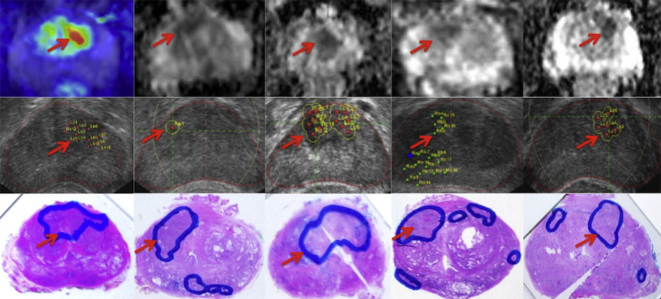
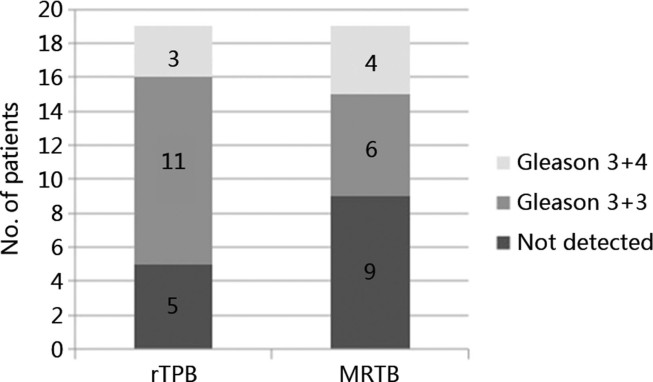
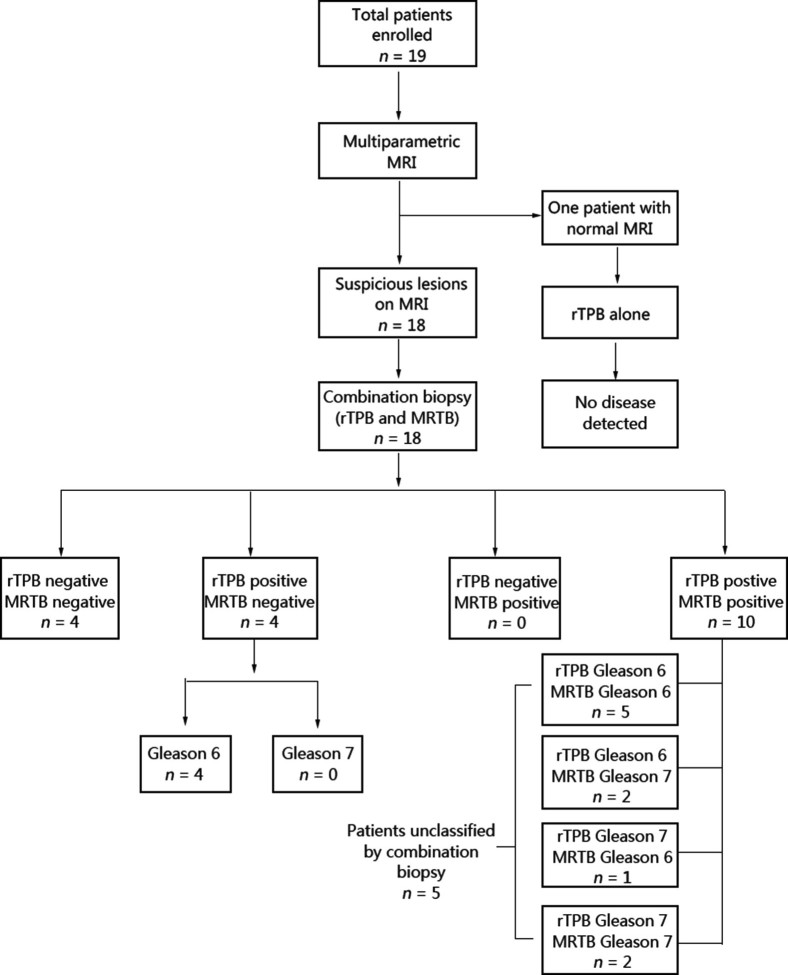
The age of the 19 men included is 65.4 ± 4.9 years (mean ± SD). Prostate specific antigen (PSA) at diagnosis and at the time of transperineal biopsy were comparable (7.3 ± 1.7 ng/mL and 7.0 ± 1.8 ng/mL, = 0.67), so were prostate volumes (34.2 ± 8.9 mL and 32.1 ± 13.4 mL, = 0.28). MRI-targeted biopsy had a higher percentage of cancer detection per core compared to template biopsy (11.7% 6.5%, = 0.02), this was more than 3 times superior for Gleason 7 disease (5.9% 1.6%, < 0.01). Four of 18 (22.2%) patients with MRI lesions had significant disease with MRI-targeted biopsy alone. Three of 19 patients (15.8%) had significant disease with template biopsy alone. In combination, both techniques upclassified five patients (26.3%), all of whom underwent radical prostatectomy. Whole mount histology confirmed tumour location and grade. All six patients with PIRADS 5 lesions had cancer detected (66.6% significant disease).
A combination of MRI-targeted and template biopsy may optimally risk-classify "low-risk" patients diagnosed on initial conventional transrectal ultrasonography (TRUS) prostate biopsy.
主动监测(AS)提供了一种减少过度治疗的策略,目前是低风险前列腺癌广泛接受的治疗选择。一种理想的风险分层工具应能检测出侵袭性癌症,并首先将这类男性排除在接受主动监测之外。我们评估经会阴模板活检与磁共振成像(MRI)靶向活检相结合是否能在最初被诊断为低风险前列腺癌的男性中识别出显著前列腺癌。
这项前瞻性、单盲研究纳入了经传统经直肠超声引导活检诊断为低风险前列腺癌(达米科标准)的男性。患者在初次活检后≥6周首先接受前列腺多参数MRI检查。对每个可疑病变进行定位并赋予前列腺影像报告和数据系统(PIRADS)评分。首先在外科医生对MRI结果不知情的情况下进行模板活检,然后使用机器人经会阴活检平台进行MRI靶向活检。
纳入的19名男性年龄为65.4±4.9岁(均值±标准差)。诊断时和经会阴活检时的前列腺特异性抗原(PSA)相当(7.3±1.7 ng/mL和7.0±1.8 ng/mL,P = 0.67),前列腺体积也相当(34.2±8.9 mL和32.1±13.4 mL,P = 0.28)。与模板活检相比,MRI靶向活检每针的癌症检出率更高(11.7%对6.5%,P = 0.02),对于 Gleason 7级疾病,前者的优势超过3倍(5.9%对1.6%,P < 0.01)。18名有MRI病变的患者中有4名(22.2%)仅通过MRI靶向活检就发现有显著疾病。19名患者中有3名(15.8%)仅通过模板活检发现有显著疾病。两种技术联合应用使5名患者(26.3%)的风险分级上调,所有这些患者均接受了根治性前列腺切除术。全切片组织学检查证实了肿瘤位置和分级。所有6名PIRADS 5级病变的患者均检测到癌症(66.6%为显著疾病)。
MRI靶向活检和模板活检相结合可能对最初经传统经直肠超声(TRUS)前列腺活检诊断为“低风险”的患者进行最佳的风险分级。