Oxford Policy Management/NHSSP, Kathmandu, Nepal.
Oxford Policy Management, Kathmandu, Nepal.
Int J Health Policy Manag. 2018 Jul 1;7(7):645-655. doi: 10.15171/ijhpm.2018.01.
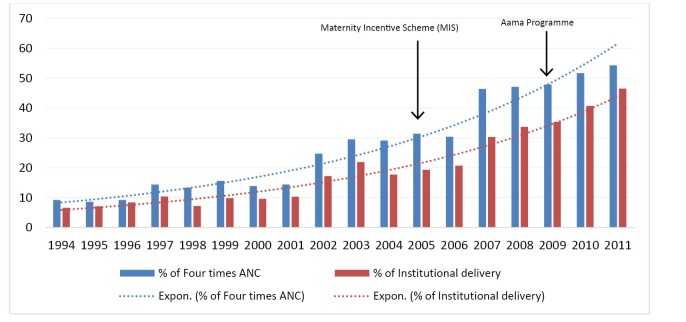
Nepal has made remarkable improvements in maternal health outcomes. The implementation of demand and supply side strategies have often been attributed with the observed increase in utilization of maternal healthcare services. In 2005, Free Delivery Care (FDC) policy was implemented under the name of Maternity Incentive Scheme (MIS), with the intention of reducing transport costs associated with giving birth in a health facility. In 2009, MIS was expanded to include free delivery services. The new expanded programme was named "Aama" programme, and further provided a cash incentive for attending four or more antenatal visits. This article analysed the influence of FDC policies, individual and community level factors in the utilisation of four antenatal care (4 ANC) visits and institutional deliveries in Nepal.
Demographic and health survey data from 1996, 2001, 2006 and 2011 were used and a multi-level analysis was employed to determine the effect of FDC policy intervention, individual and community level factors in utilisation of 4 ANC visits and institutional delivery services.
Multivariate analysis suggests that FDC policy had the largest effect in the utilisation of 4 ANC visits and institutional delivery compared to individual and community factors. After the implementation of MIS in 2005, women were three times (adjusted odds ratio [AOR]=3.020, P<.001) more likely to attend 4 ANC visits than when there was no FDC policy. After the implementation of Aama programme in 2009, the likelihood of attending 4 ANC visits increased six-folds (AOR=6.006, P<.001) compared prior to the implementation of FDC policy. Similarly, institutional deliveries increased two times after the implementation of the MIS (AOR=2.117, P<.001) than when there was no FDC policy. The institutional deliveries increased five-folds (AOR=5.116, P<.001) after the implementation of Aama compared to no FDC policy.
Results from this study suggest that MIS and Aama policies have had a strong positive influence on the utilisation of 4 ANC visits and institutional deliveries in Nepal. Nevertheless, results also show that FDC policies may not be sufficient in raising demand for maternal health services without adequately considering the individual and community level factors.
尼泊尔在改善母婴健康结果方面取得了显著进步。需求和供应方策略的实施通常归因于观察到的母婴保健服务利用率的提高。2005 年,免费分娩护理(FDC)政策以产妇激励计划(MIS)的名义实施,旨在降低在医疗机构分娩的相关交通成本。2009 年,MIS 扩大到包括免费分娩服务。新的扩展方案被命名为"Aama"计划,并进一步为参加四次或更多次产前检查提供现金奖励。本文分析了尼泊尔 FDC 政策、个人和社区层面因素对四次产前护理(4ANC)就诊和机构分娩利用率的影响。
使用 1996 年、2001 年、2006 年和 2011 年的人口与健康调查数据,并采用多水平分析确定 FDC 政策干预、个人和社区层面因素对 4ANC 就诊和机构分娩服务利用的影响。
多变量分析表明,与个人和社区因素相比,FDC 政策对 4ANC 就诊和机构分娩的利用影响最大。2005 年 MIS 实施后,与没有 FDC 政策时相比,妇女参加 4ANC 就诊的可能性增加了三倍(调整后的优势比[AOR]=3.020,P<.001)。2009 年 Aama 计划实施后,与实施 FDC 政策之前相比,参加 4ANC 就诊的可能性增加了六倍(AOR=6.006,P<.001)。同样,MIS 实施后(AOR=2.117,P<.001),机构分娩次数增加了两倍,而没有 FDC 政策时则没有。与没有 FDC 政策相比,Aama 实施后机构分娩增加了五倍(AOR=5.116,P<.001)。
本研究结果表明,MIS 和 Aama 政策对尼泊尔 4ANC 就诊和机构分娩的利用产生了强烈的积极影响。然而,结果还表明,在不充分考虑个人和社区层面因素的情况下,FDC 政策可能不足以提高对母婴保健服务的需求。