Department of Pathology, Cancer Center Amsterdam, VU University Medical Center, Amsterdam, The Netherlands.
DDL Diagnostic Laboratory, Rijswijk, The Netherlands.
J Clin Pathol. 2018 Nov;71(11):981-988. doi: 10.1136/jclinpath-2018-205271. Epub 2018 Jul 16.
To investigate the accuracy and reproducibility of a scoring system for cervical intraepithelial neoplasia (CIN1-3) based on immunohistochemical (IHC) biomarkers Ki-67 and p16.
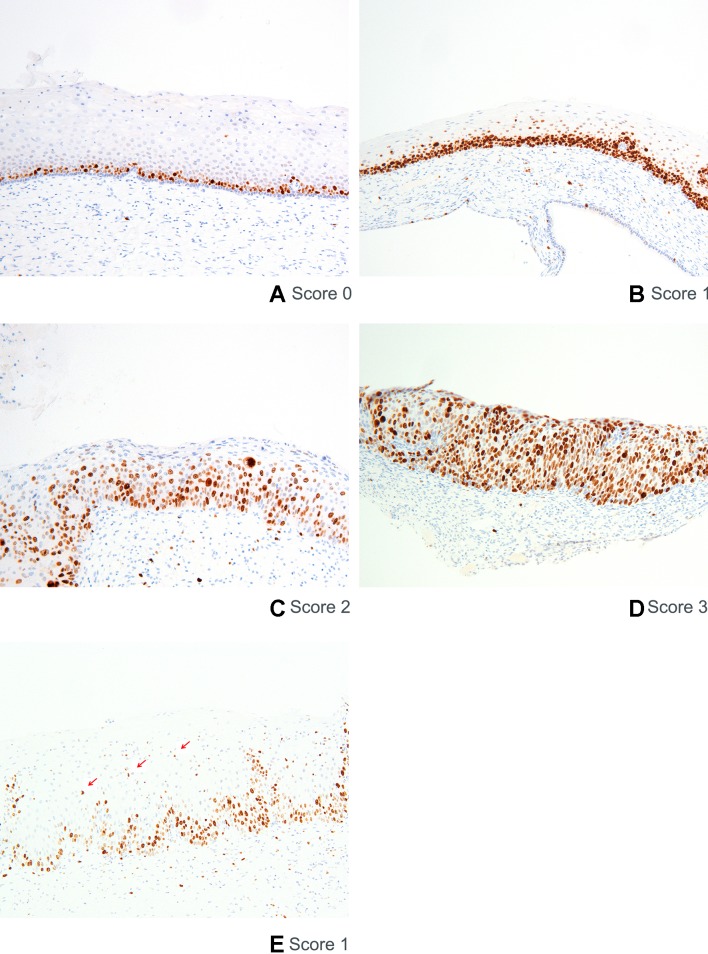
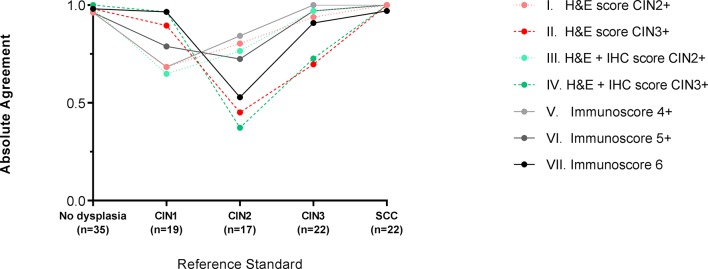
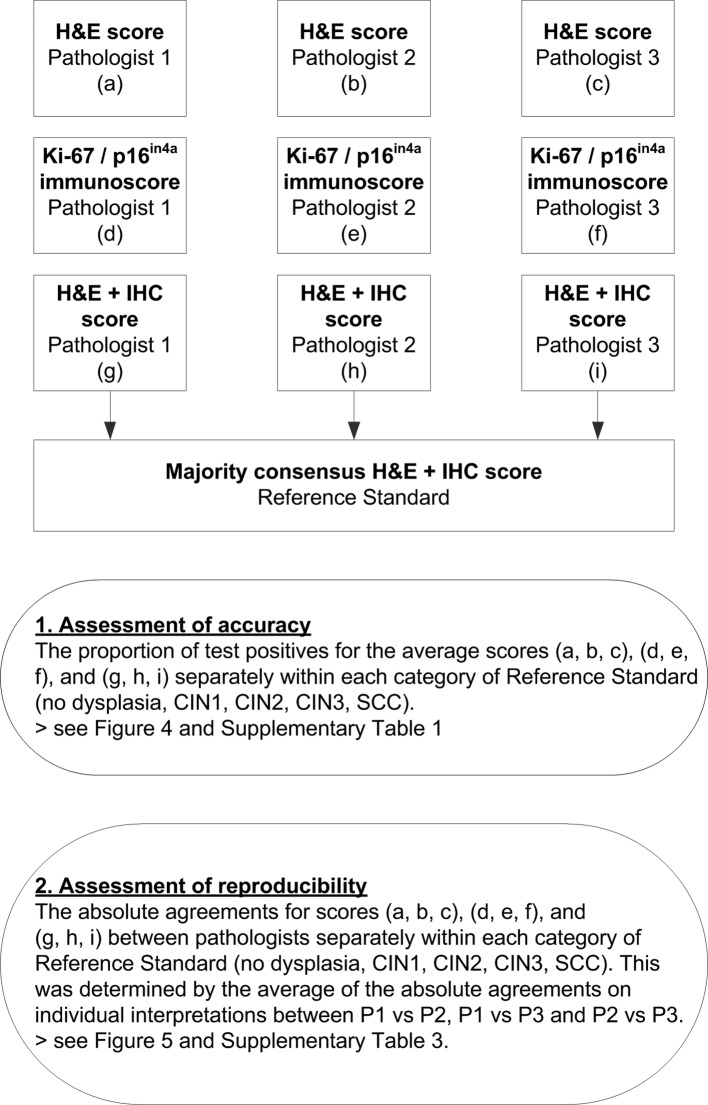
115 cervical tissue specimens were reviewed by three expert gynaecopathologists and graded according to three strategies: (1) CIN grade based on H&E staining only; (2) immunoscore based on the cumulative score of Ki-67 and p16 only (0-6); and (3) CIN grade based on H&E supported by non-objectified IHC 2 weeks after scoring 1 and 2. The majority consensus diagnosis of the CIN grade based on H&E supported by IHC was used as the . The proportion of test positives () and the absolute agreements across pathologists () of the three grading strategies within each category were calculated.
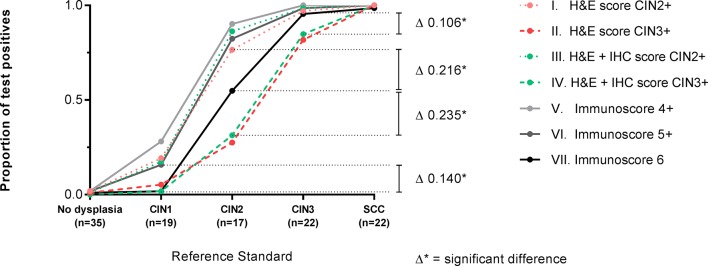
We found that immunoscoring with positivity definition 6 yielded the highest proportion of test positives for (95.5%), in combination with the lowest proportion of test positives in samples with (1.8%). The proportion of test positives for was significantly lower for sole H&E staining (81.8%) or combined H&E and IHC grading (84.8%) with positivity definition ≥CIN3. Immunoscore 6 also yielded high absolute agreements for and , but the absolute agreement was low for .
The higher accuracy and reproducibility of the immunoscore opens the possibility of a more standardised and reproducible definition of CIN grade than conventional pathology practice, allowing a more accurate comparison of CIN-based management strategies and evaluation of new biomarkers to improve the understanding of progression of precancer from human papillomavirus infection to cancer.
研究基于免疫组织化学(IHC)生物标志物 Ki-67 和 p16 的宫颈上皮内瘤变(CIN1-3)评分系统的准确性和可重复性。
回顾了 115 例宫颈组织标本,由 3 位妇科病理学家进行评估,并根据三种策略进行分级:(1)仅基于 H&E 染色的 CIN 分级;(2)仅基于 Ki-67 和 p16 累积评分的免疫评分(0-6);(3)基于 H&E 分级,在评分 1 和 2 后 2 周支持非客观 IHC。使用基于 H&E 支持 IHC 的多数共识诊断 CIN 分级作为参考标准。计算每种 CIN 分级策略的测试阳性比例()和病理学家之间的绝对一致率()。
我们发现,阳性定义为 6 的免疫评分可获得最高的测试阳性比例(95.5%),同时在 CIN 分级为 1 的样本中测试阳性比例最低(1.8%)。仅基于 H&E 染色(81.8%)或联合 H&E 和 IHC 分级(84.8%)的测试阳性比例明显低于阳性定义≥CIN3。免疫评分 6 还为和 提供了较高的绝对一致率,但对的绝对一致率较低。
免疫评分的准确性和可重复性更高,为比传统病理学实践更标准化和可重复的 CIN 分级定义提供了可能性,从而可以更准确地比较基于 CIN 的管理策略,并评估新的生物标志物,以提高对人乳头瘤病毒感染到癌症进展的癌前病变的理解。