Heart and Vascular Center; Noninvasive Cardiovascular Imaging Program, Departments of Medicine (Cardiology) and Radiology (Nuclear Medicine and Molecular Imaging), Brigham and Women's Hospital, Harvard Medical School, Boston, MA, USA.
Adv Exp Med Biol. 2018;1065:257-278. doi: 10.1007/978-3-319-77932-4_17.
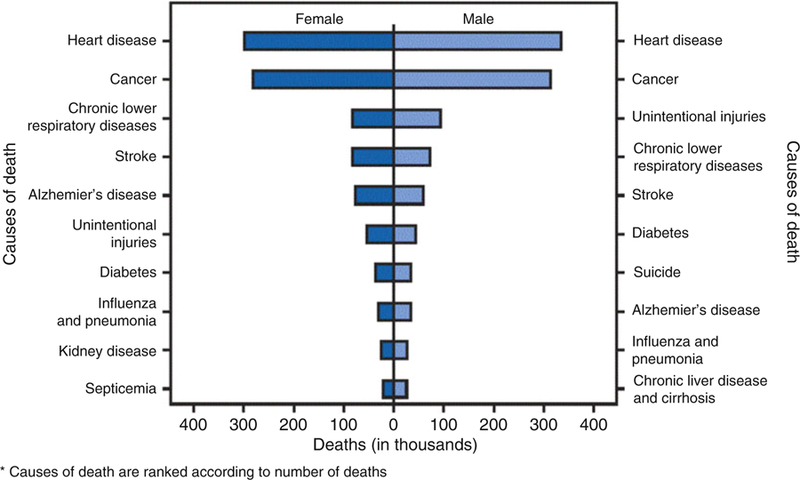
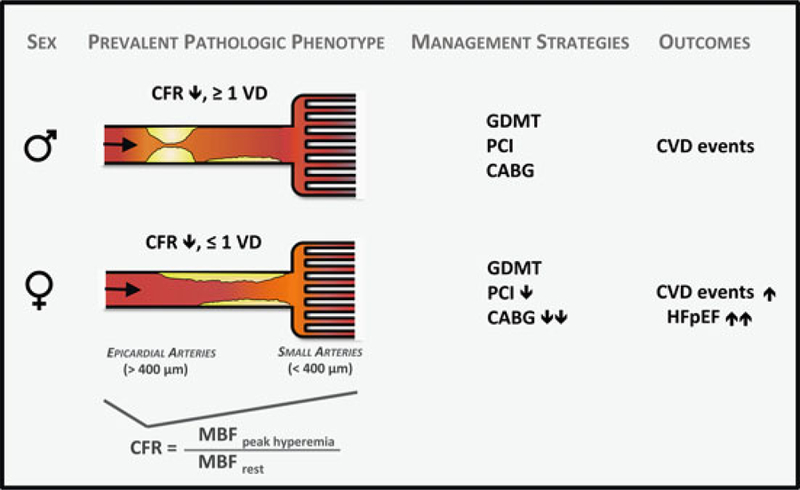
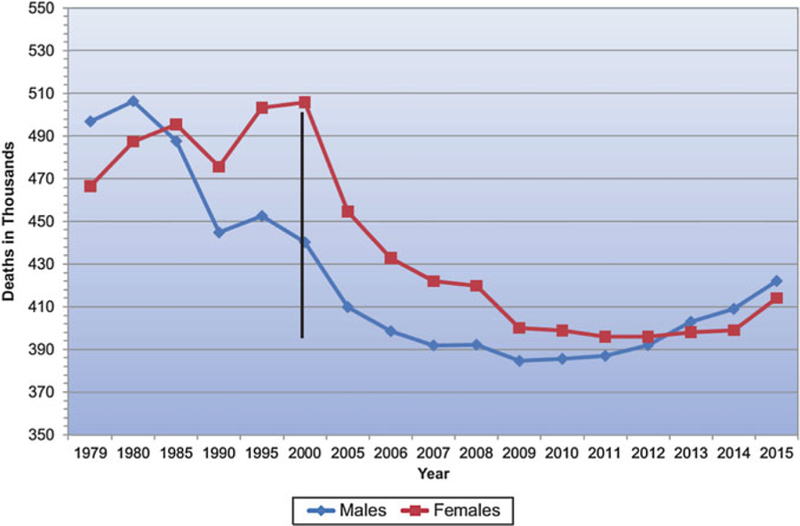
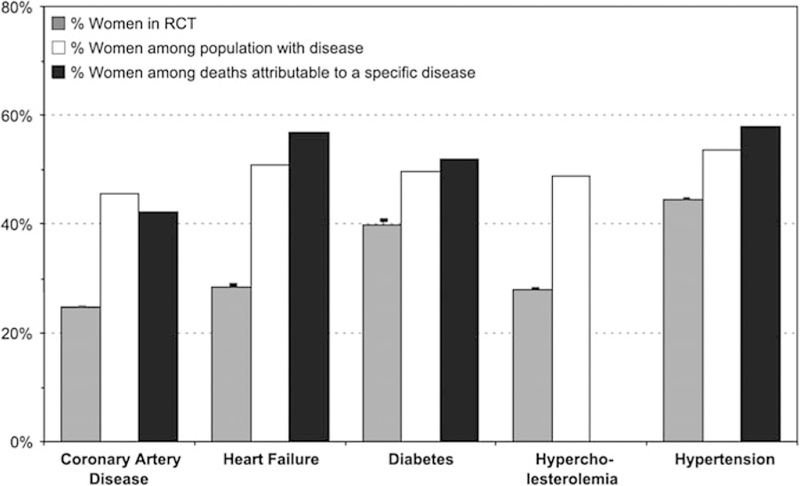
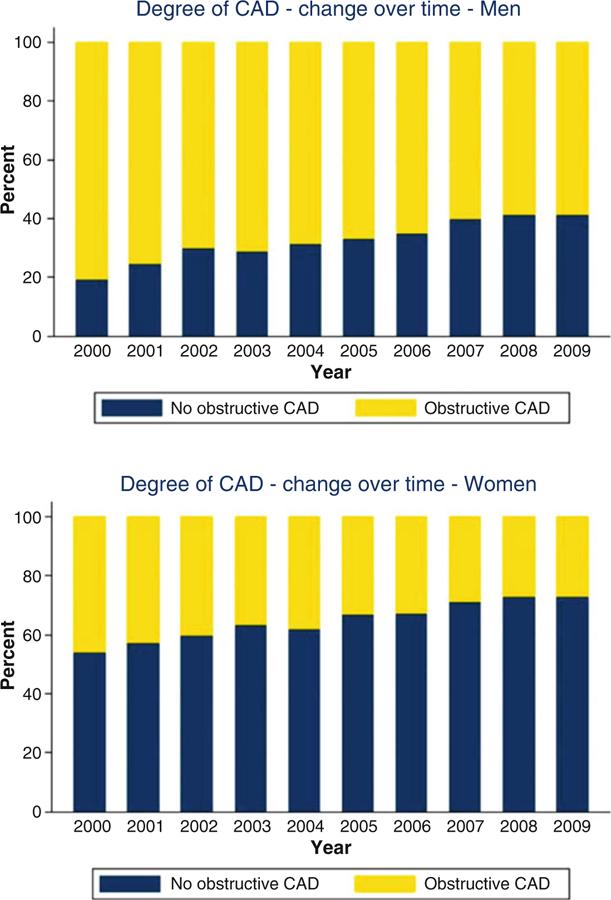
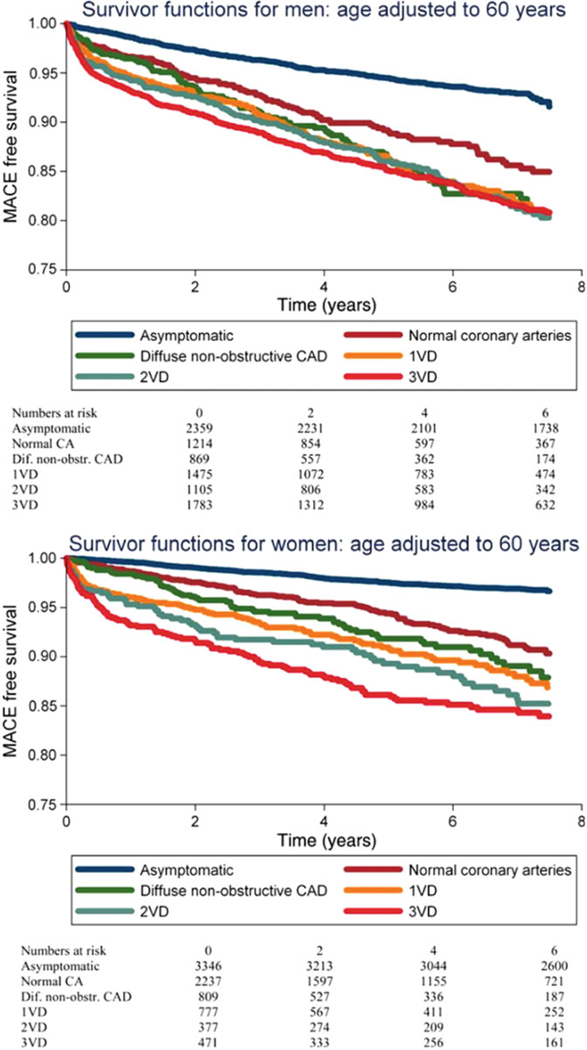
Cardiovascular disease remains the leading cause of morbidity and mortality for both women and men. Emerging evidence supports that ischemic heart disease (IHD) may manifest differently in women and men, in ways ranging from the clinical presentation, diagnosis, and management of disease to the basic biology and biomechanics of cardiomyocyte function and the coronary circulation. Women consistently present with a higher burden of symptoms and comorbidities as compared with men and experience worse outcomes. These data have proved perplexing given the decreased likelihood of women to demonstrate obstructive coronary artery disease (CAD) on coronary angiography. Reported sex differences have long been influenced by the practice of defining heart disease primarily as obstructive CAD, but obstructive plaque is now recognized as neither necessary nor sufficient to explain symptoms of IHD, and it is no longer adequate to tailor diagnostic and treatment strategies only to this subset of patients. To date, women remain underrepresented in guideline-changing heart disease research and trials, creating important limitations in the evidence base for cardiovascular medicine. Smaller epicardial coronary arteries in women as compared to men, coupled with differences in shear stress and inflammatory mediators over the life span, may modify the development of CAD in susceptible patients into a diffuse pattern with more contribution from coronary vasomotor dysfunction than focal obstruction. Newer studies corroborate that symptomatic women are more likely than men to present with nonobstructive CAD and coronary microvascular dysfunction. When present, these processes increase cardiovascular risk in both women and men but may constitute an especially malignant phenotype in a subset of severely affected women, with implications for the management of not only CAD but also heart failure with preserved ejection fraction. This represents a state-of-the-art review of sex differences in the coronary system, with an eye toward how diverse pathophysiological processes may contribute to IHD phenotypes prevalent in women and men. Beyond providing women and men with equitable optimal care according to current paradigms, understanding the pathophysiology of IHD beyond a conventional focus on obstructive CAD is needed to address what is likely a combination of biological as well as environmental determinants of their prognosis.
心血管疾病仍然是女性和男性发病率和死亡率的主要原因。新出现的证据支持,缺血性心脏病(IHD)在女性和男性中的表现可能不同,从临床表现、疾病诊断和治疗到心肌细胞功能和冠状动脉循环的基本生物学和生物力学等方面。与男性相比,女性的症状和合并症负担更高,结局更差。这些数据令人费解,因为女性在冠状动脉造影上显示阻塞性冠状动脉疾病(CAD)的可能性降低。长期以来,报告的性别差异一直受到将心脏病主要定义为阻塞性 CAD 的实践的影响,但现在已经认识到阻塞性斑块既不是解释 IHD 症状的必要条件,也不是充分条件,仅针对这部分患者制定诊断和治疗策略已经不再足够。迄今为止,女性在改变心脏病研究和试验的指南方面仍然代表性不足,这为心血管医学的证据基础带来了重要限制。与男性相比,女性的心脏外膜冠状动脉较小,加上一生中剪切应力和炎症介质的差异,可能会使易感患者的 CAD 发展为弥漫性模式,而不是局灶性阻塞,更多地归因于冠状动脉血管舒缩功能障碍。新的研究证实,有症状的女性比男性更有可能出现非阻塞性 CAD 和冠状动脉微血管功能障碍。当这些情况存在时,它们会增加女性和男性的心血管风险,但在一部分严重受影响的女性中可能构成一种特别恶性的表型,这对不仅 CAD 而且射血分数保留的心力衰竭的治疗都有影响。这是对冠状动脉系统性别差异的最新综述,着眼于不同的病理生理过程如何导致女性和男性中常见的 IHD 表型。除了根据当前范式为女性和男性提供平等的最佳护理外,还需要超越传统的关注阻塞性 CAD 来理解 IHD 的病理生理学,以解决可能是他们预后的生物学和环境决定因素的组合。