Triadafilopoulos George, Clarke John O
Stanford Esophageal Multi-disciplinary Program in Innovative Research Excellence (SEMPIRE), Division of Gastroenterology and Hepatology, Stanford University School of Medicine, Stanford, California, USA.
BMJ Open Gastroenterol. 2018 Jul 25;5(1):e000210. doi: 10.1136/bmjgast-2018-000210. eCollection 2018.
The Chicago Classification (CC) defines oesophagogastric junction outflow obstruction (EGJOO) as the presence of an elevated integrated residual pressure (IRP) together with preserved oesophageal body peristalsis but its clinical significance is evolving.
To describe the clinical and manometric characteristics in patients with EGJOO and propose a new classification.
In this retrospective cohort study, patients with functional oesophageal symptoms underwent clinical and endoscopic assessment and oesophageal high-resolution manometry (HRM). The CC V.3 was used to define and redefine abnormalities.
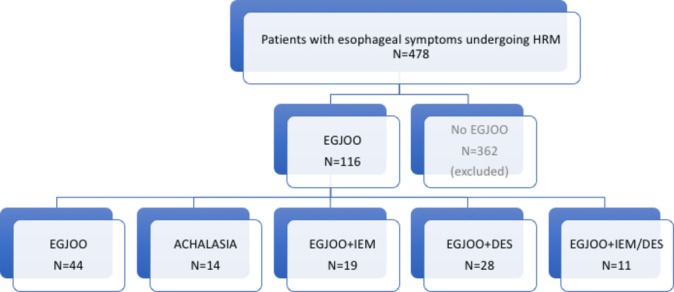
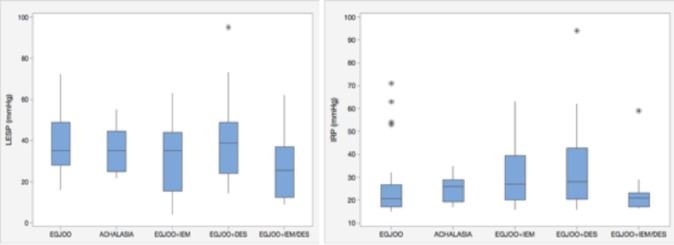
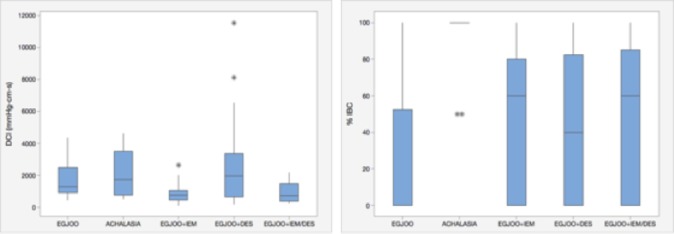
Of 478 HRM studies performed, EGJOO, defined as median IRP >15 mm Hg, was diagnosed in 116 patients; 17 underwent a follow-up HRM. Forty-four patients had otherwise normal oesophageal motility, with the only finding being EGJOO; 14 had achalasia, 19 had EGJOO plus ineffective oesophageal motility (IEM), 28 had EGJOO plus diffuse oesophageal spasm (DES) (n=25) or jackhammer oesophagus (n=3), and 11 had EGJOO plus IEM and DES. Patients with EGJOO+IEM had lower distal contractile integral (DCI) while those with EGJOO+DES had higher DCI. All groups exhibited high percentages of incomplete bolus clearance. On repeat studies, EGJOO preceded or followed another HRM diagnosis and remained permanent in 2/17 patients. Only one patient transitioned to achalasia.
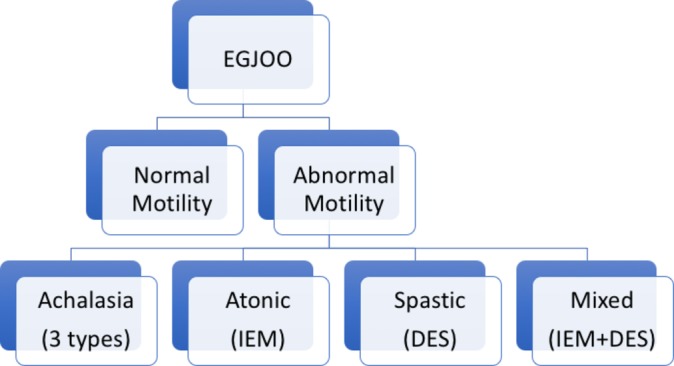
The new classification further defines EGJOO by considering abnormalities in the body of the oesophagus that could contribute to symptoms or require therapy. Most patients with EGJOO have a coexisting motility disorder and do not have isolated EGJOO. There is a fluidity of the HRM diagnosis that needs to be considered prior to therapy.
芝加哥分类法(CC)将食管胃交界部流出道梗阻(EGJOO)定义为综合残余压力(IRP)升高且食管体部蠕动保留,但它的临床意义仍在不断演变。
描述EGJOO患者的临床和测压特征并提出一种新的分类方法。
在这项回顾性队列研究中,有功能性食管症状的患者接受了临床和内镜评估以及食管高分辨率测压(HRM)。采用CC V.3来定义和重新定义异常情况。
在进行的478项HRM研究中,116例患者被诊断为EGJOO(定义为IRP中位数>15 mmHg);17例接受了随访HRM。44例患者食管动力其他方面正常,唯一发现是EGJOO;14例患有贲门失弛缓症,19例患有EGJOO加无效食管动力(IEM),28例患有EGJOO加弥漫性食管痉挛(DES)(n = 25)或胡桃夹食管(n = 3),11例患有EGJOO加IEM和DES。EGJOO + IEM患者的远端收缩积分(DCI)较低,而EGJOO + DES患者的DCI较高。所有组均显示出较高比例的食团清除不完全。在重复研究中,EGJOO先于或后于另一种HRM诊断出现,并且在17例患者中的2例中持续存在。只有1例患者转变为贲门失弛缓症。
新的分类方法通过考虑食管体部可能导致症状或需要治疗的异常情况,进一步定义了EGJOO。大多数EGJOO患者存在并存的动力障碍,并非孤立的EGJOO。HRM诊断存在动态变化,在治疗前需要考虑这一点。