Ibrahim Jamil, Hazzan Azzour D, Mathew Anna T, Sakhiya Vipul, Zhang Meng, Halinski Candice, Fishbane Steven
Division of Nephrology, Department of Medicine, Hofstra Northwell School of Medicine, Great Neck, NY, USA.
Clin Kidney J. 2018 Aug;11(4):507-512. doi: 10.1093/ckj/sfx135. Epub 2017 Nov 23.
Late-stage chronic kidney disease (LS-CKD) can be defined by glomerular filtration rate (GFR) 0-30 mL/min. It is a period of risk for medication discrepancies because of frequent hospitalizations, fragmented medical care, inadequate communication and polypharmacy. In this study, we sought to characterize medication discrepancies in LS-CKD.
We analyzed all patients enrolled in Northwell Health's Healthy Transitions in LS-CKD program. All patients had estimated GFR 0-30 mL/min, not on dialysis. Medications were reviewed by a nurse at a home visit. Patients' medication usage and practice were compared with nephrologists' medication lists, and discrepancies were characterized. Patients were categorized as having either no discrepancies or one or more. Associations between patient characteristics and number of medication discrepancies were evaluated by chi-square or Fisher's exact test for categorical variables, and two-sample -test or Wilcoxon text for continuous variables.
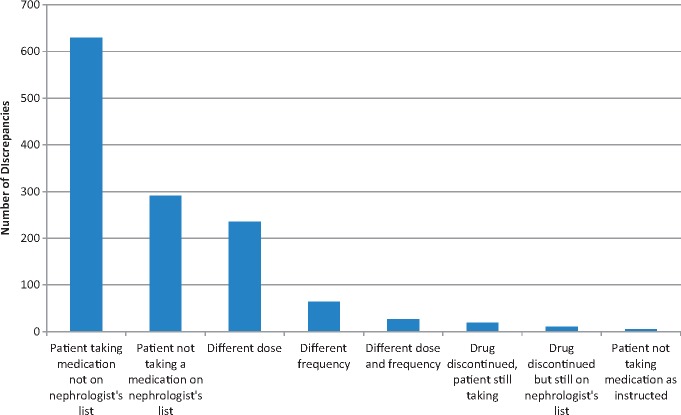
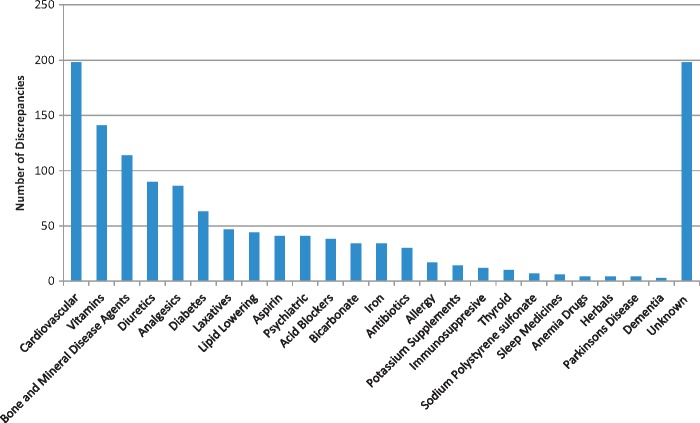
Seven hundred and thirteen patients with a median age of 70 (interquartile range 58-79) years were studied. There were 392 patients (55.0% of the study population) with at least one medication discrepancy. The therapeutic classes of medications with most frequently occurring medication discrepancies were cardiovascular, vitamins, bone and mineral disease agents, diuretics, analgesics and diabetes medications. In multivariable analysis, factors associated with higher risk of discrepancies were congestive heart failure [odds ratio (OR) 2.13; 95% confidence interval (CI) 1.44-3.16; P = 0.0002] and number of medications (OR 1.29; 95% CI 1.21-1.37; P < 0.0001).
Medication discrepancies are common in LS-CKD, affect the majority of patients and include high-risk medication classes. Congestive heart failure and total number of medications are independently associated with greater risk for multiple drug discrepancies. The frequency of medication discrepancies indicates a need for great care in medication management of these patients.
晚期慢性肾脏病(LS-CKD)可定义为肾小球滤过率(GFR)为0至30毫升/分钟。由于频繁住院、医疗服务碎片化、沟通不足和多重用药,这一时期存在用药差异风险。在本研究中,我们试图描述LS-CKD患者的用药差异情况。
我们分析了所有参与诺斯韦尔健康中心LS-CKD项目“健康过渡”的患者。所有患者的估算肾小球滤过率为0至30毫升/分钟,且未接受透析治疗。护士在家庭访视时对患者的用药情况进行了审查。将患者的用药情况和用药习惯与肾病科医生的用药清单进行比较,并对差异进行描述。患者被分为无差异或有一个或多个差异两类。通过卡方检验或费舍尔精确检验评估分类变量的患者特征与用药差异数量之间的关联,通过两样本t检验或威尔科克森检验评估连续变量之间的关联。
共研究了713例患者,中位年龄为70岁(四分位间距58至79岁)。有392例患者(占研究人群的55.0%)至少存在一处用药差异。用药差异最常出现的治疗类别药物为心血管药物、维生素、骨与矿物质疾病药物、利尿剂、镇痛药和糖尿病药物。在多变量分析中,与差异风险较高相关的因素为充血性心力衰竭[比值比(OR)2.13;95%置信区间(CI)1.44至3.16;P = 0.0002]和用药数量(OR 1.29;95% CI 1.21至1.37;P < 0.0001)。
用药差异在LS-CKD患者中很常见,影响大多数患者,且涉及高风险药物类别。充血性心力衰竭和用药总数与多种药物差异的较高风险独立相关。用药差异的频率表明在这些患者的用药管理中需要格外谨慎。