Al-Eid Raniah Abdullah, Ramalingam Sundar, Sundar Chalini, Aldawsari Mona, Nooh Nasser
Department of Oral and Maxillofacial Surgery, College of Dentistry, King Saud University, Riyadh, Saudi Arabia.
Department of Research Support, College of Dentistry, King Saud University, Riyadh, Saudi Arabia.
J Int Soc Prev Community Dent. 2018 Jul-Aug;8(4):327-332. doi: 10.4103/jispcd.JISPCD_10_18. Epub 2018 Jul 18.
Oral surgical procedures can cause spread of infections in the clinics through visually imperceptible, splattered, and aerosolized blood. The aim of this study was to evaluate visually imperceptible blood contamination of clinical surfaces and personal protective equipment (PPE) in an oral surgery clinic using luminol.
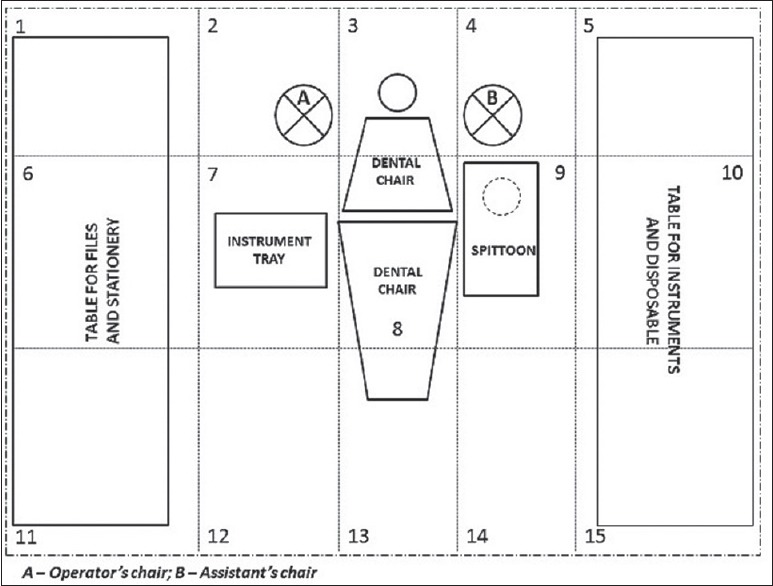
Following ethical approval, oral surgical procedures were performed under local anesthesia in a disinfected clinic, and PPE was used by the oral surgeon, dental assistant, and patients. After the procedure, clinical surfaces and PPE were evaluated for traces of visually imperceptible blood contamination using luminol. Data regarding blood contamination and the duration of the procedure were collected. Nonparametric tests, with 95% significance level (Epi Info, Stat Calc 7, CDC, Atlanta, USA), were used to identify statistical interactions between the duration of the procedure and the frequency of blood contamination.
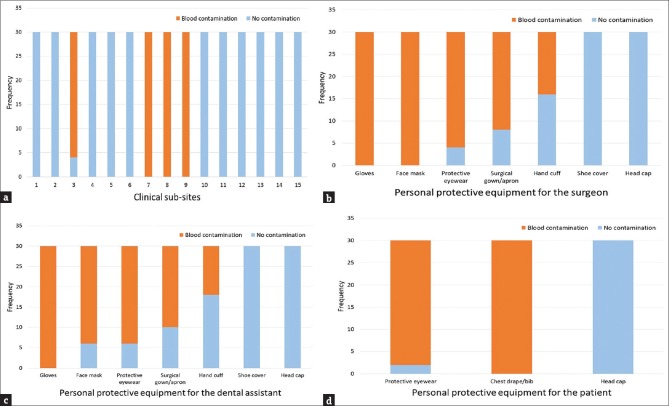
Blood contamination was detected in flooring below surgical field (86.67%), instrument tray, operating light, dental chair, and suction unit (100%). Except head caps and shoe covers, blood contamination was detected in all the PPE used by the clinical personnel, and the eyewear and chest drapes used by patients. An increase in the surgical time beyond 40 min significantly increased the risk of blood contamination in the handcuffs of the clinical personnel ( < 0.01).
Visually imperceptible blood contamination of the clinical surfaces and PPE is associated with minor oral surgical procedures. This mandates the cleaning and disinfection of all clinical surfaces before and after minor oral surgical procedures and PPE for clinicians and patients during every procedure.
口腔外科手术可能会通过肉眼难以察觉的、飞溅的和气溶胶化的血液在诊所内传播感染。本研究的目的是使用鲁米诺评估口腔外科诊所中临床表面和个人防护装备(PPE)上肉眼难以察觉的血液污染情况。
在获得伦理批准后,在消毒后的诊所内进行局部麻醉下的口腔外科手术,口腔外科医生、牙科助手和患者均使用个人防护装备。手术后,使用鲁米诺评估临床表面和个人防护装备上肉眼难以察觉的血液污染痕迹。收集有关血液污染和手术持续时间的数据。使用具有95%显著性水平的非参数检验(美国亚特兰大疾病控制与预防中心的Epi Info,Stat Calc 7)来确定手术持续时间与血液污染频率之间的统计相关性。
在手术区域下方的地板上检测到血液污染(86.67%),器械托盘、手术灯、牙科椅和吸引装置上均检测到血液污染(100%)。除了头罩和鞋套外,临床人员使用的所有个人防护装备以及患者使用的眼镜和胸部手术巾上均检测到血液污染。手术时间超过40分钟会显著增加临床人员手铐上血液污染的风险(<0.01)。
临床表面和个人防护装备上肉眼难以察觉的血液污染与小型口腔外科手术有关。这就要求在小型口腔外科手术前后对所有临床表面进行清洁和消毒,并在每次手术期间为临床医生和患者提供个人防护装备。