The Royal Melbourne Hospital, Parkville, Australia.
Department of Diabetes and Endocrinology, The Royal Melbourne Hospital, Parkville, VIC, 3050, Australia.
Mol Med. 2018 May 30;24(1):27. doi: 10.1186/s10020-018-0028-3.
Parathyroid glands of people with relapsing remitting multiple sclerosis (RRMS) fail to respond to low serum 25-hydroxyvitamin D (25OHD) and low serum calcium, which are stimuli for parathyroid hormone (PTH) secretion. This led us to hypothesise: that there is suppression of PTH in RRMS due to higher than normal serum concentrations of fibroblast growth factor 23 (FGF23). We therefore sought evidence for dysregulation of the PTH-FGF23-vitamin D axis in RRMS.
Longitudinal study (winter to summer) with fasting venepunctures. For RRMS subjects who recruited a healthy control (HC) friend, pairs analyses were performed. For each pair, the within-pair difference of the variable of interest was calculated (RRMS minus HC). Then, the median of the differences from all pairs was compared against a median of zero (Wilcoxon) and the 95% confidence interval of that median difference (CI) was calculated (Sign Test).
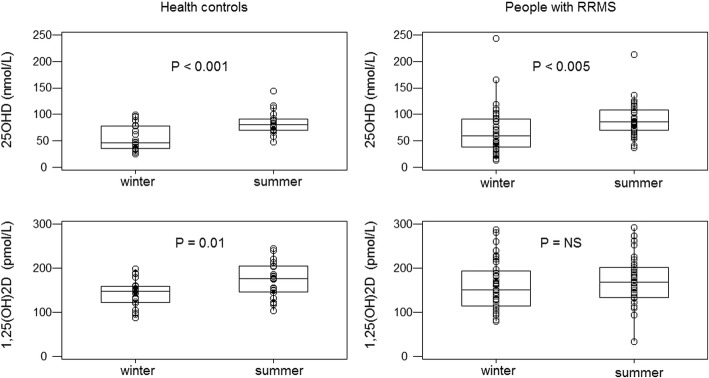
RRMS had lower winter PTH than HC, P = 0.005, (CI -2.4 to 0.5 pmol/L, n = 28 pairs), and lower summer PTH, P = 0.04, (CI -1.8 to 0.5, n = 21 pairs). Lower PTH associates physiologically with lower intact FGF23 (iFGF23), yet RRMS had higher iFGF23 than HC in winter, P = 0.04, (CI -3 to 15 pg/mL, n = 28 pairs) and iFGF23 levels comparable to HC in summer, P = 0.14, (CI -5 to 13, n = 21 pairs). As PTH stimulates and FGF23 reduces, renal 1-alpha hydroxylase enzyme activity, which synthesises serum 1,25-dihyroxyvitamin D (1,25(OH)D) from serum 25OHD, we examined the ratio of serum 1,25(OH)D to serum 25OHD. In winter, this ratio was lower in RRMS versus HC, P = 0.013, (CI -1.2 to - 0.3, n = 28 pairs).
This study revealed a dysequilibrium of the PTH-FGF23-vitamin D axis in RRMS, with lower plasma PTH, higher plasma iFGF23 and a lower serum 1,25(OH)D to 25OHD ratio in RRMS compared with HC subjects. This dysequilibrium is consistent with the study hypothesis that in RRMS there is suppression of the parathyroid glands by inappropriately high plasma concentrations of iFGF23. Studying the basis of this dysequilibrium may provide insight into the pathogenesis of RRMS.
复发缓解型多发性硬化症(RRMS)患者的甲状旁腺对低血清 25-羟维生素 D(25OHD)和低血清钙无反应,而低血清钙和 25OHD 是甲状旁腺激素(PTH)分泌的刺激物。这使我们假设:RRMS 中 PTH 受到抑制是由于血清成纤维细胞生长因子 23(FGF23)浓度高于正常水平。因此,我们试图寻找 RRMS 中 PTH-FGF23-维生素 D 轴失调的证据。
冬季至夏季进行空腹静脉穿刺的纵向研究。对于招募了健康对照(HC)朋友的 RRMS 受试者,进行了配对分析。对于每对,计算了感兴趣变量的内对差异(RRMS 减去 HC)。然后,将所有配对差异的中位数与中位数为零(Wilcoxon)进行比较,并计算中位数差异的 95%置信区间(CI)(Sign 检验)。
RRMS 的冬季 PTH 低于 HC,P=0.005(CI-2.4 至 0.5 pmol/L,n=28 对),夏季 PTH 也较低,P=0.04(CI-1.8 至 0.5,n=21 对)。较低的 PTH 与较低的完整成纤维细胞生长因子 23(iFGF23)生理相关,但 RRMS 的冬季 iFGF23 高于 HC,P=0.04(CI-3 至 15 pg/mL,n=28 对),夏季 iFGF23 与 HC 相当,P=0.14(CI-5 至 13,n=21 对)。由于 PTH 刺激,FGF23 降低,肾脏 1-α羟化酶活性降低,该酶将血清 25OHD 转化为血清 1,25-二羟维生素 D(1,25(OH)D),我们检查了血清 1,25(OH)D 与血清 25OHD 的比值。在冬季,RRMS 与 HC 相比,该比值较低,P=0.013(CI-1.2 至-0.3,n=28 对)。
这项研究揭示了 RRMS 中 PTH-FGF23-维生素 D 轴的失衡,与 HC 受试者相比,RRMS 患者的血浆 PTH 较低,血浆 iFGF23 较高,血清 1,25(OH)D 与 25OHD 的比值较低。这种失衡与研究假设一致,即 RRMS 中甲状旁腺受到不适当高的血浆 iFGF23 浓度的抑制。研究这种失衡的基础可能为 RRMS 的发病机制提供新的见解。