Levintow Sara N, Okeke Nwora Lance, Hué Stephane, Mkumba Laura, Virkud Arti, Napravnik Sonia, Sebastian Joseph, Miller William C, Eron Joseph J, Dennis Ann M
Department of Epidemiology, University of North Carolina, Chapel Hill, North Carolina.
Division of Infectious Diseases, Duke University, Durham, North Carolina.
Open Forum Infect Dis. 2018 Jul 20;5(8):ofy178. doi: 10.1093/ofid/ofy178. eCollection 2018 Aug.
Transmitted drug resistance (TDR) compromises clinical management and outcomes. Transmitted drug resistance surveillance and identification of growing transmission clusters are needed in the Southeast, the epicenter of the US HIV epidemic. Our study investigated prevalence and transmission dynamics in North Carolina.
We analyzed surveillance drug resistance mutations (SDRMs) using partial sequences from patients presenting to 2 large HIV outpatient clinics from 1997 to 2014. Transmitted drug resistance prevalence was defined as ≥1 SDRMs among antiretroviral therapy (ART)-naïve patients. Binomial regression was used to characterize prevalence by calendar year, drug class, and demographic and clinical factors. We assessed the transmission networks of patients with TDR with maximum likelihood trees and Bayesian methods including background sequences (n = 15 246).
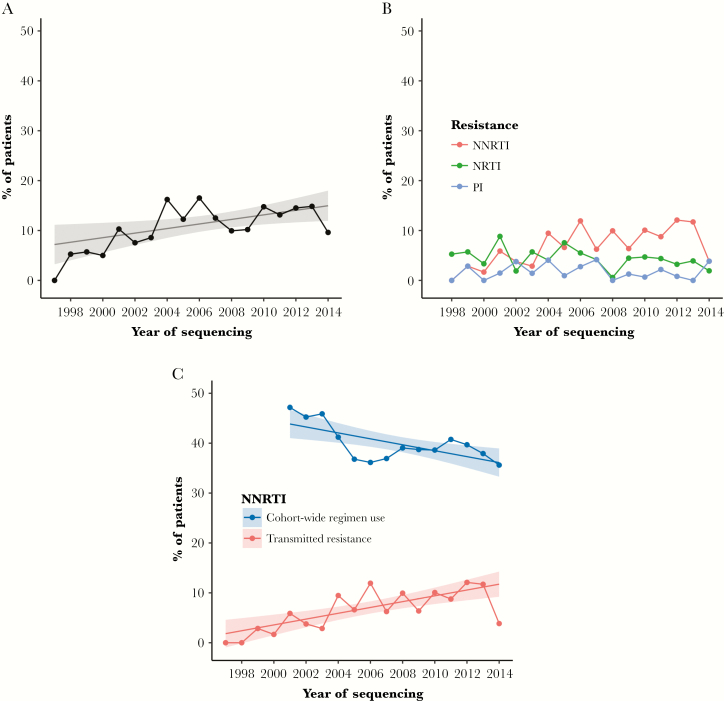
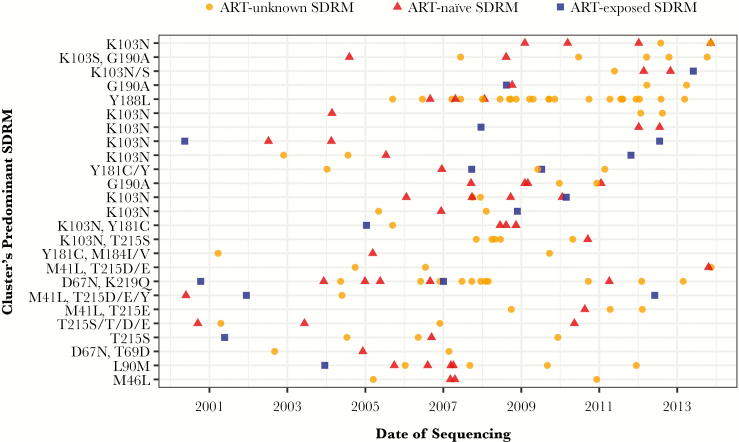
Among 1658 patients with pretherapy resistance testing, ≥1 SDRMs was identified in 199 patients, with an aggregate TDR prevalence of 12% (95% confidence interval, 10% to 14%) increasing over time ( = .02). Resistance to non-nucleoside reverse transcriptase inhibitors (NNRTIs; 8%) was common, followed by nucleoside reverse transcriptase inhibitors (4%) and protease inhibitors (2%). Factors associated with TDR were being a man reporting sex with men, white race, young age, higher CD4 cell count, and being a member of a transmission cluster. Transmitted drug resistance was identified in 106 clusters ranging from 2 to 26 members. Cluster resistance was primarily NNRTI and dominated by ART-naïve patients or those with unknown ART initiation.
Moderate TDR prevalence persists in North Carolina, predominantly driven by NNRTI resistance. Most TDR cases were identified in transmission clusters, signifying multiple local transmission networks and TDR circulation among ART-naïve persons. Transmitted drug resistance surveillance can detect transmission networks and identify patients for enhanced services to promote early treatment.
传播性耐药(TDR)会影响临床管理和治疗结果。美国艾滋病流行的中心在东南部,因此需要对该地区进行传播性耐药监测并识别不断扩大的传播集群。我们的研究调查了北卡罗来纳州的流行率和传播动态。
我们使用了1997年至2014年期间到两家大型艾滋病门诊就诊患者的部分序列,分析了监测耐药突变(SDRM)。传播性耐药流行率定义为未接受抗逆转录病毒治疗(ART)的患者中存在≥1个SDRM。采用二项式回归按日历年、药物类别以及人口统计学和临床因素来描述流行率特征。我们用最大似然树和贝叶斯方法(包括15246条背景序列)评估了传播性耐药患者的传播网络。
在1658例接受治疗前耐药检测的患者中,199例患者被鉴定出≥1个SDRM,总体传播性耐药流行率为12%(95%置信区间为10%至14%),且随时间增加(P = 0.02)。对非核苷类逆转录酶抑制剂(NNRTI;8%)的耐药很常见,其次是核苷类逆转录酶抑制剂(4%)和蛋白酶抑制剂(2%)。与传播性耐药相关 的因素包括男性、报告有男男性行为、白人种族、年轻、CD4细胞计数较高以及属于一个传播集群。在106个集群中发现了传播性耐药,集群成员数从2人到26人不等。集群耐药主要是对NNRTI的耐药,且主要发生在未接受ART治疗的患者或开始接受ART治疗情况不明的患者中。
北卡罗来纳州持续存在中度传播性耐药流行,主要由对NNRTI的耐药所致。大多数传播性耐药病例在传播集群中被发现,这表明存在多个本地传播网络以及在未接受ART治疗的人群中存在传播性耐药的循环。传播性耐药监测可以检测传播网络并识别患者,以便提供强化服务以促进早期治疗。