Division of Cardiology, Department of Medicine, Duke University Medical Center, Durham, NC, USA.
Duke Clinical Research Institute, Durham, NC, USA.
Eur J Heart Fail. 2019 Jan;21(1):63-70. doi: 10.1002/ejhf.1299. Epub 2018 Aug 31.
A 5-point change in the Kansas City Cardiomyopathy Questionnaire (KCCQ) is commonly considered to be a clinically significant difference in health status in patients with heart failure. We evaluated how the magnitude of change relates to subsequent clinical outcomes.
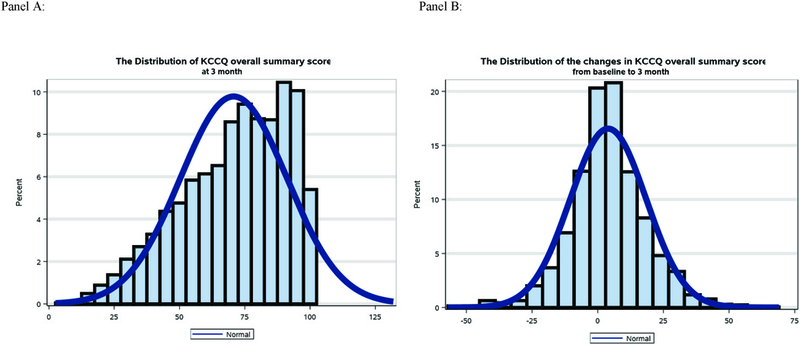
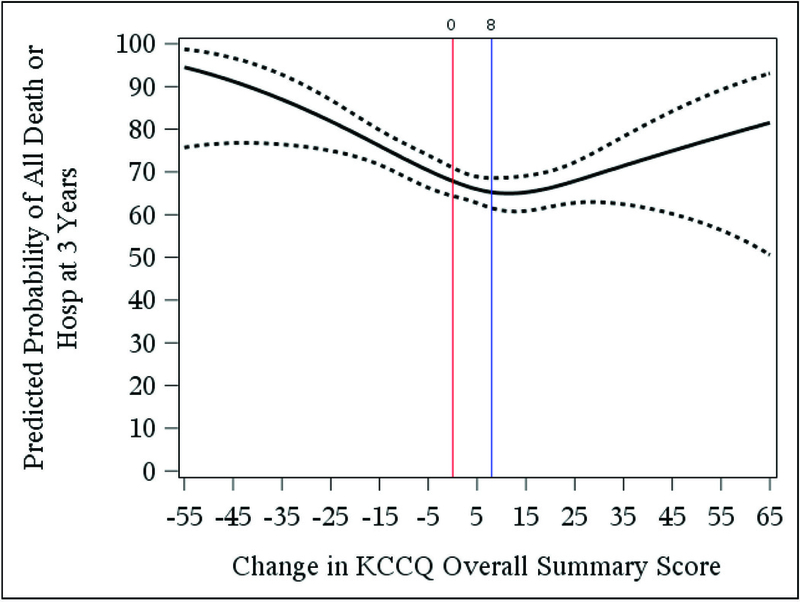
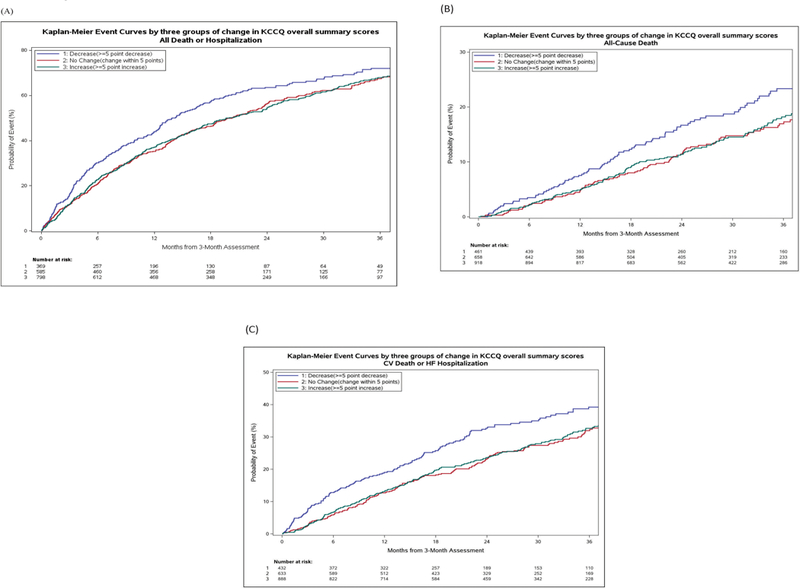
Using data from the HF-ACTION trial of exercise training in chronic heart failure (n = 2331), we used multivariable Cox regression with piecewise linear splines to examine the relationship between change in KCCQ overall summary score from baseline to 3 months (range 0-100; higher scores reflect better health status) and subsequent all-cause mortality/hospitalization. Among 2038 patients with KCCQ data at the 3-month visit, KCCQ scores increased from baseline by ≥5 points for 45%, scores decreased by ≥5 points for 23%, and scores changed by <5 points for the remaining 32% of patients. There was a non-linear relationship between change in KCCQ and outcomes. Worsening health status was associated with increased all-cause mortality/hospitalization (adjusted hazard ratio 1.07 per 5-point KCCQ decline; 95% confidence interval 1.03-1.12; P < 0.001). In contrast, improving health status, up to an 8-point increase in KCCQ, was associated with decreased all-cause mortality/hospitalization (adjusted hazard ratio 0.93 per 5-point increase; 95% confidence interval 0.90-0.97; P < 0.001). Additional improvements in health status beyond an 8-point increase in KCCQ was not associated with all-cause death or hospitalization (P = 0.42).
In patients with heart failure, small changes in KCCQ are associated with changing future risk, but more research will be necessary to understand how different magnitudes of improving health status affect outcomes.
堪萨斯城心肌病问卷(KCCQ)的 5 分变化通常被认为是心力衰竭患者健康状况的临床显著差异。我们评估了变化幅度与随后临床结局的关系。
使用来自慢性心力衰竭运动训练 HF-ACTION 试验的数据(n=2331),我们使用多变量 Cox 回归与分段线性样条来检查从基线到 3 个月时 KCCQ 总评分变化(范围 0-100;得分越高表示健康状况越好)与随后的全因死亡率/住院之间的关系。在 2038 名在 3 个月就诊时具有 KCCQ 数据的患者中,KCCQ 评分≥5 分的患者增加了 45%,评分下降≥5 分的患者占 23%,而其余 32%的患者评分变化<5 分。KCCQ 变化与结局之间存在非线性关系。健康状况恶化与全因死亡率/住院增加相关(调整后的危险比为 KCCQ 每下降 5 分增加 1.07;95%置信区间为 1.03-1.12;P<0.001)。相比之下,健康状况改善,KCCQ 增加 8 分,与全因死亡率/住院减少相关(调整后的危险比为 KCCQ 每增加 5 分降低 0.93;95%置信区间为 0.90-0.97;P<0.001)。KCCQ 增加超过 8 分后健康状况的进一步改善与全因死亡或住院无关(P=0.42)。
在心力衰竭患者中,KCCQ 的微小变化与未来风险的变化相关,但需要进一步研究以了解健康状况改善的不同幅度如何影响结局。