Blok Joris J, Putter Hein, Metselaar Herold J, Porte Robert J, Gonella Federica, de Jonge Jeroen, van den Berg Aad P, van der Zande Josephine, de Boer Jacob D, van Hoek Bart, Braat Andries E
Division of Transplantation, Department of Surgery, Leiden University Medical Center, Leiden University, Leiden, the Netherlands.
Department of Medical Statistics, Leiden University Medical Center, Leiden University, Leiden, the Netherlands.
Transplant Direct. 2018 Aug 21;4(9):e382. doi: 10.1097/TXD.0000000000000822. eCollection 2018 Sep.
Outcome after liver transplantation (LT) is determined by donor, transplant and recipient risk factors. These factors may have different impact on either patient or graft survival (outcome type). In the literature, there is wide variation in the use of outcome types and points in time (short term or long term). Objective of this study is to analyze the predictive capacity of risk factors and risk models in LT and how they vary over time and per outcome type.
All LTs performed in the Netherlands from January 1, 2002, to December 31, 2011, were analyzed with multivariate analyses at 3-month, 1-year, and 5-year for patient and (non-)death-censored graft survival. The predictive capacity of the investigated risk models was compared with concordance indices.
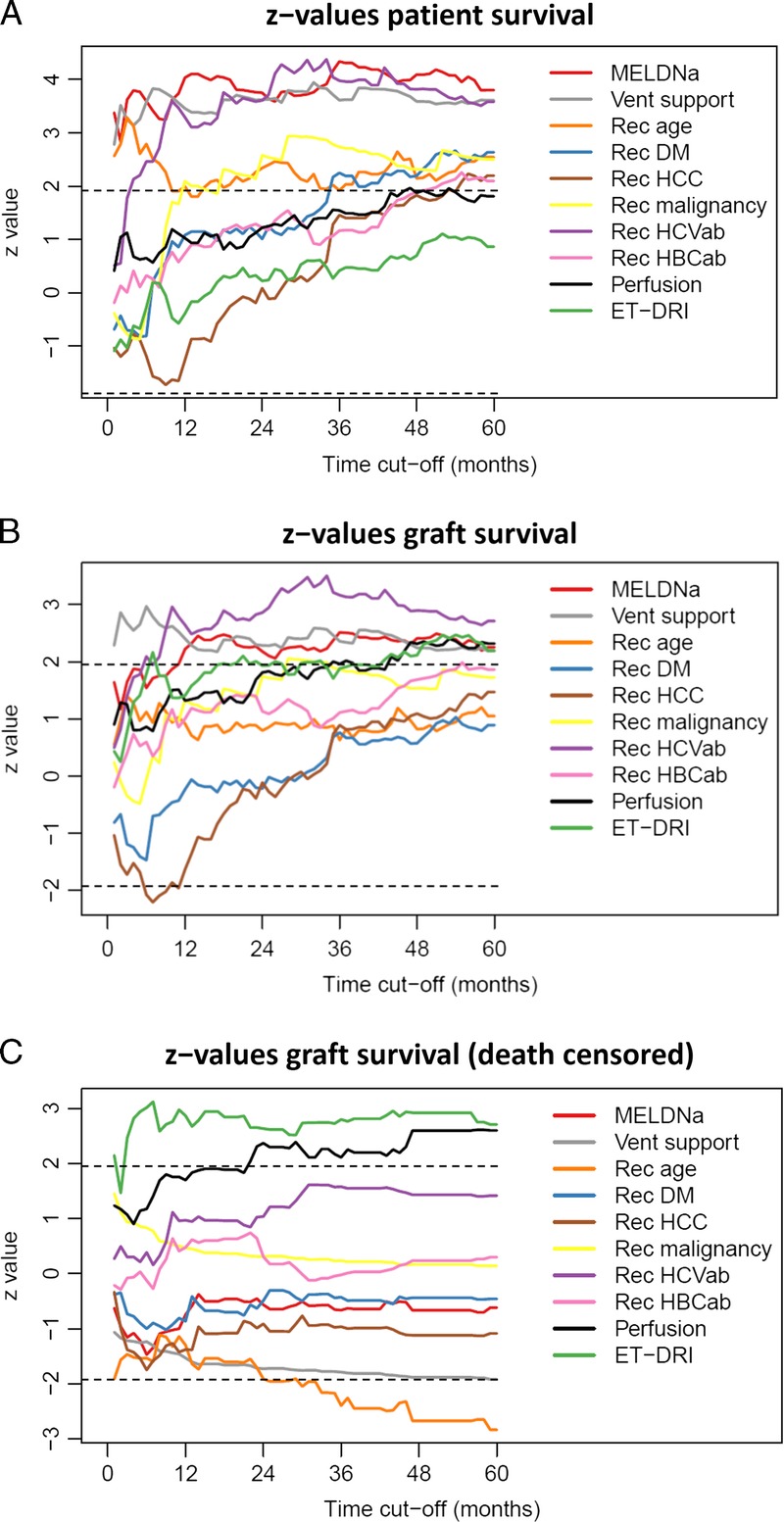
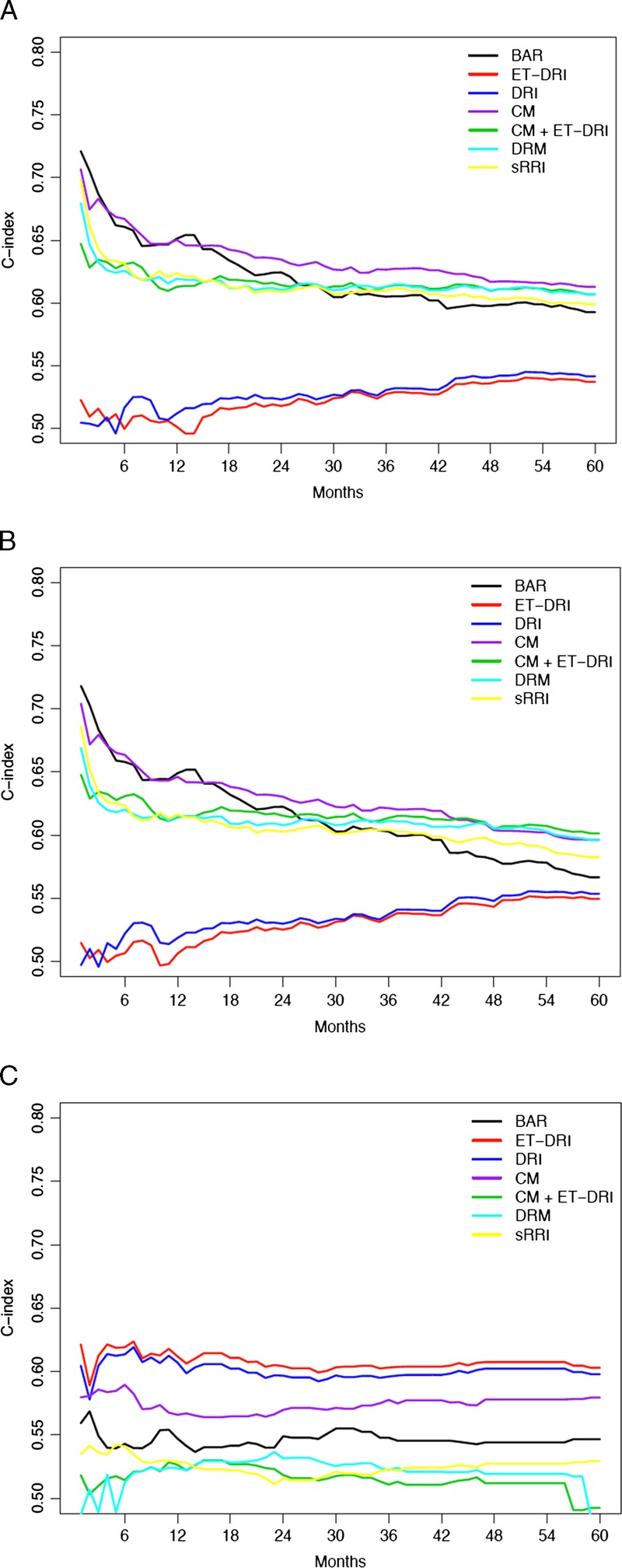
Recipient age, model for end-stage liver disease sodium, ventilatory support, diabetes mellitus, hepatocellular carcinoma, previous malignancy, hepatitis C virus antibody, hepatitis B virus antibody, perfusion fluid, and Eurotransplant donor risk index (ET-DRI) had significant impact on outcome (graft or patient survival) at 1 or multiple points in time. Significant factors at 3-month patient survival (recipient age, model for end-stage liver disease sodium, ventilatory support) were used to compose a concept model. This model, had a higher c-index than the balance-of-risk score, DRI, ET-DRI, donor-recipient model and simplified recipient risk index for long-term patient and non-death-censored graft survival.
In this study, the effects of recipient risk factors and models on different outcome types and time points were shown. Short-term patient survival mainly depends on recipient risk factors, long-term graft survival on donor risk factors and is more difficult to predict. Next to the concept model, the donor-recipient model has a higher predictive capacity to other risk models for (long-term) patient and non-death-censored graft survival. The DRI and ET-DRI best predicted death-censored graft survival. Knowledge about risk factors and models is critical when using these for waitlist management and/or help in organ allocation and decision-making.
肝移植(LT)后的结局由供体、移植和受体风险因素决定。这些因素对患者或移植物存活(结局类型)可能有不同影响。在文献中,结局类型和时间点(短期或长期)的使用存在很大差异。本研究的目的是分析LT中风险因素和风险模型的预测能力,以及它们如何随时间和结局类型而变化。
对2002年1月1日至2011年12月31日在荷兰进行的所有肝移植进行多变量分析,分别在3个月、1年和5年时分析患者及(非)死亡删失的移植物存活情况。将所研究风险模型的预测能力与一致性指数进行比较。
受体年龄、终末期肝病钠模型、通气支持、糖尿病、肝细胞癌、既往恶性肿瘤、丙型肝炎病毒抗体、乙型肝炎病毒抗体、灌注液和欧洲移植供体风险指数(ET-DRI)在1个或多个时间点对结局(移植物或患者存活)有显著影响。用于构建概念模型的3个月患者存活的显著因素(受体年龄、终末期肝病钠模型、通气支持)。该模型在长期患者和非死亡删失的移植物存活方面,其c指数高于风险平衡评分、供体风险指数、ET-DRI、供体-受体模型和简化受体风险指数。
本研究显示了受体风险因素和模型对不同结局类型和时间点的影响。短期患者存活主要取决于受体风险因素,长期移植物存活取决于供体风险因素且更难预测。除概念模型外,供体-受体模型对(长期)患者和非死亡删失的移植物存活的预测能力高于其他风险模型。DRI和ET-DRI对死亡删失的移植物存活预测最佳。在将这些用于等待名单管理和/或帮助进行器官分配及决策时,了解风险因素和模型至关重要。