Rutgers Cancer Institute of New Jersey, New Brunswick, New Jersey.
Urologic Oncology Program, Division of Urology, Department of Surgery, Rutgers Robert Wood Johnson Medical School, New Brunswick, New Jersey.
Cancer. 2018 Oct 15;124(20):4010-4022. doi: 10.1002/cncr.31726. Epub 2018 Sep 25.
Men with locally advanced prostate cancer (LAPCa) or regionally advanced prostate cancer (RAPCa) are at high risk for death from their disease. Clinical guidelines support multimodal approaches, which include radical prostatectomy (RP) followed by radiotherapy (XRT) and XRT plus androgen deprivation therapy (ADT). However, there are limited data comparing these substantially different treatment approaches. Using Surveillance, Epidemiology, and End Results (SEER)-Medicare data, this study compared survival outcomes and adverse effects associated with RP plus XRT versus XRT plus ADT in these men.
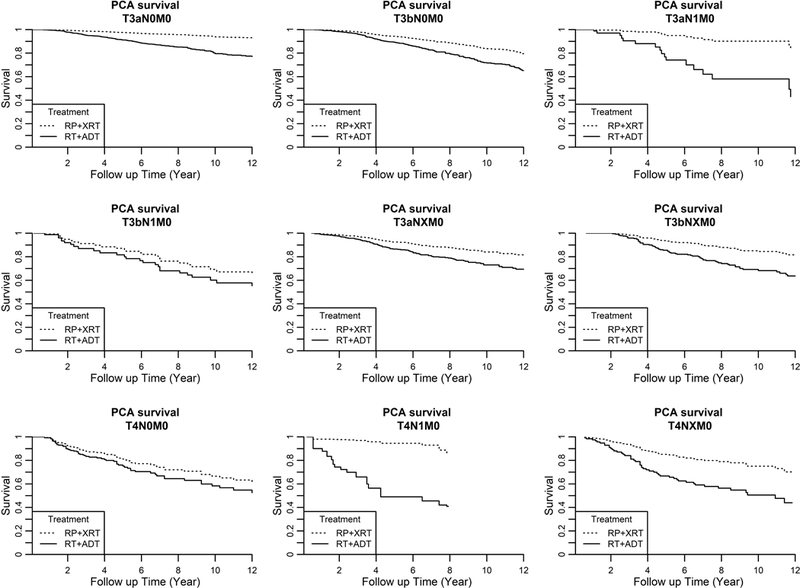
SEER-Medicare data were queried for men with cT3-T4N0M0 (LAPCa) or cT3-T4N1M0 (RAPCa) prostate cancer. Propensity score methods were used to balance cohort characteristics between the treatment arms. Survival analyses were analyzed with the Kaplan-Meier method and Cox proportional hazards models.
From 1992 to 2009, 13,856 men (≥65 years old) were diagnosed with LAPCa or RAPCa: 6.1% received RP plus XRT, and 23.6% received XRT plus ADT. At a median follow-up of 14.6 years, there were 2189 deaths in the cohort, of which 702 were secondary to prostate cancer. Regardless of the tumor stage or the Gleason score, the adjusted 10-year prostate cancer-specific survival and 10-year overall survival favored men who underwent RP plus XRT over men who underwent XRT plus ADT. However, RP plus XRT versus XRT plus ADT was associated with higher rates of erectile dysfunction (28% vs 20%; P = .0212) and urinary incontinence (49% vs 19%; P < .001).
Men with LAPCa or RAPCa treated initially with RP plus XRT had a lower risk of prostate cancer-specific death and improved overall survival in comparison with those men treated with XRT plus ADT, but they experienced higher rates of erectile dysfunction and urinary incontinence.
局部晚期前列腺癌(LAPCa)或局部区域进展性前列腺癌(RAPCa)患者死于该疾病的风险较高。临床指南支持多模式方法,包括根治性前列腺切除术(RP)后放疗(XRT)和 XRT 加雄激素剥夺疗法(ADT)。然而,比较这些差异很大的治疗方法的数据有限。本研究使用监测、流行病学和最终结果(SEER)-医疗保险数据,比较了这些患者中 RP 加 XRT 与 XRT 加 ADT 治疗的生存结果和不良反应。
使用 SEER-医疗保险数据查询 cT3-T4N0M0(LAPCa)或 cT3-T4N1M0(RAPCa)前列腺癌患者。使用倾向评分方法平衡治疗组之间的队列特征。使用 Kaplan-Meier 方法和 Cox 比例风险模型分析生存分析。
1992 年至 2009 年,共有 13856 名(≥65 岁)男性被诊断为 LAPCa 或 RAPCa:6.1%接受 RP 加 XRT,23.6%接受 XRT 加 ADT。在中位随访 14.6 年后,队列中有 2189 人死亡,其中 702 人死于前列腺癌。无论肿瘤分期或 Gleason 评分如何,接受 RP 加 XRT 的男性与接受 XRT 加 ADT 的男性相比,调整后的 10 年前列腺癌特异性生存率和 10 年总生存率都有优势。然而,RP 加 XRT 与 XRT 加 ADT 相比,与更高的勃起功能障碍发生率(28%比 20%;P=0.0212)和尿失禁发生率(49%比 19%;P<0.001)相关。
与接受 XRT 加 ADT 的患者相比,初始接受 RP 加 XRT 治疗的 LAPCa 或 RAPCa 患者死于前列腺癌特异性死亡的风险较低,总生存状况得到改善,但勃起功能障碍和尿失禁的发生率较高。