Health Informatics, University Hospitals Birmingham NHS Foundation Trust, Birmingham, UK.
Institute of Applied Health Research, University of Birmingham, Birmingham, UK.
BMJ Qual Saf. 2019 Mar;28(3):223-230. doi: 10.1136/bmjqs-2018-008219. Epub 2018 Oct 9.
To determine whether the higher weekend admission mortality risk is attributable to increased severity of illness.
Retrospective analysis of 4 years weekend and weekday adult emergency admissions to a university teaching hospital in England.
30-day postadmission weekend:weekday mortality ratios adjusted for severity of illness (baseline National Early Warning Score (NEWS)), routes of admission to hospital, transfer to the intensive care unit (ICU) and demographics.
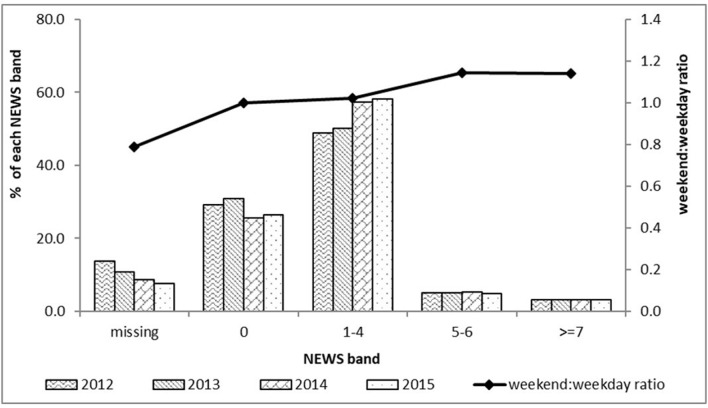
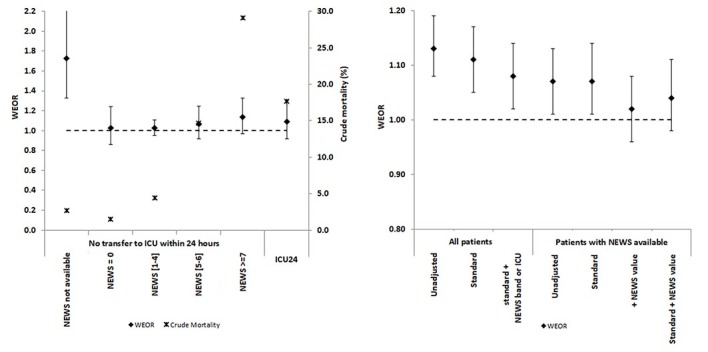
Despite similar emergency department daily attendance rates, fewer patients were admitted on weekends (mean admission rate 91/day vs 120/day) because of fewer general practitioner referrals. Weekend admissions were sicker than weekday (mean NEWS 1.8 vs 1.7, p=0.008), more likely to undergo transfer to ICU within 24 hours (4.2% vs 3.0%), spent longer in hospital (median 3 days vs 2 days) and less likely to experience same-day discharge (17.2% vs 21.9%) (all p values <0.001).The crude 30-day postadmission mortality ratio for weekend admission (OR=1.13; 95% CI 1.08 to 1.19) was attenuated using standard adjustment (OR=1.11; 95% CI 1.05 to 1.17). In patients for whom NEWS values were available (90%), the crude OR (1.07; 95% CI 1.01 to 1.13) was not affected with standard adjustment. Adjustment using NEWS alone nullified the weekend effect (OR=1.02; 0.96-1.08).NEWS completion rates were higher on weekends (91.7%) than weekdays (89.5%). Missing NEWS was associated with direct transfer to intensive care bypassing electronic data capture. Missing NEWS in non-ICU weekend patients was associated with a higher mortality and fewer same-day discharges than weekdays.
Patients admitted to hospital on weekends are sicker than those admitted on weekdays. The cause of the weekend effect may lie in community services.
确定周末入院死亡率较高是否归因于疾病严重程度的增加。
对英国一所大学教学医院 4 年周末和工作日成年急诊入院进行回顾性分析。
30 天内周末:经疾病严重程度调整后的周末:工作日死亡率比(基线国家早期预警评分(NEWS))、入院途径、转入重症监护病房(ICU)和人口统计学。
尽管急诊部每日就诊率相似,但由于全科医生转诊较少,周末入院人数较少(平均入院率为 91/天 vs 120/天)。周末入院患者病情较严重(平均 NEWS 为 1.8 vs 1.7,p=0.008),更有可能在 24 小时内转入 ICU(4.2% vs 3.0%),住院时间更长(中位数为 3 天 vs 2 天),出院率较低(17.2% vs 21.9%)(所有 p 值均<0.001)。周末入院的 30 天死亡率比值为 1.13(95%CI 1.08 至 1.19),经标准调整后减弱(比值为 1.11;95%CI 1.05 至 1.17)。在 NEWS 值可用的患者中(90%),未经调整的粗比值(1.07;95%CI 1.01 至 1.13)不受影响。仅使用 NEWS 进行调整消除了周末效应(比值为 1.02;0.96 至 1.08)。周末 NEWS 完成率(91.7%)高于工作日(89.5%)。缺少 NEWS 与直接转入重症监护病房绕过电子数据采集有关。非 ICU 周末患者缺少 NEWS 与死亡率较高和较少的当日出院有关。
周末入院的患者比工作日入院的患者病情更严重。周末效应的原因可能在于社区服务。