Department of Radiology and Nuclear Medicine, Erasmus Medical Center, P.O. Box 2240, 3000 CA, Rotterdam, The Netherlands.
Eur Radiol. 2019 Apr;29(4):2079-2088. doi: 10.1007/s00330-018-5745-z. Epub 2018 Oct 10.
To assess the accuracy of a 3D camera for body contour detection and patient positioning in CT compared to routine manual positioning by radiographers.
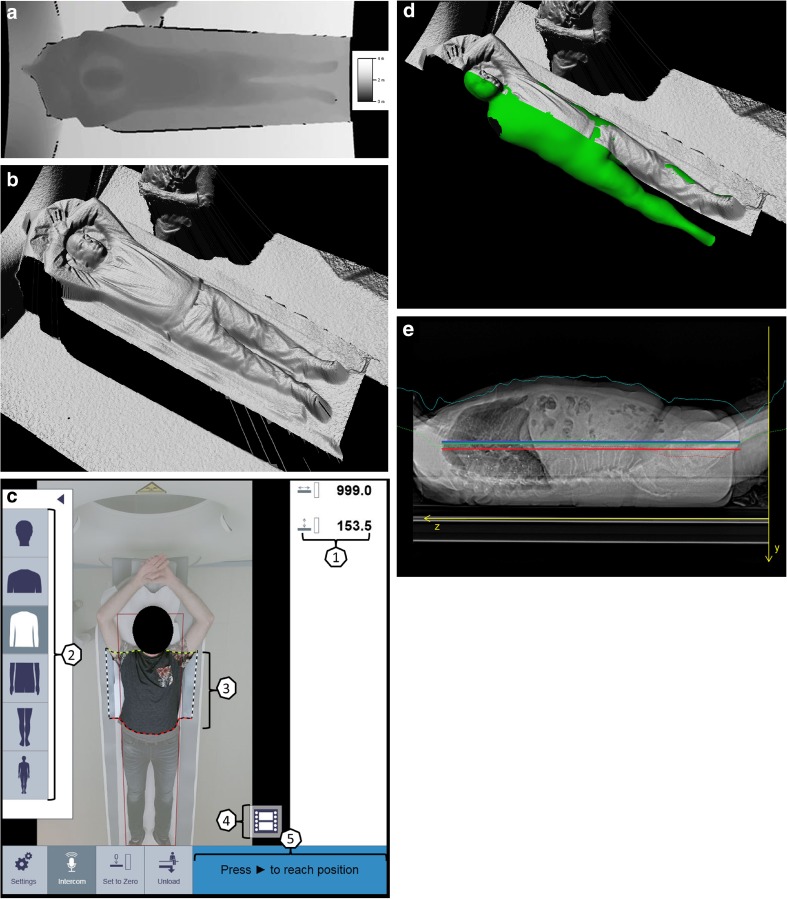
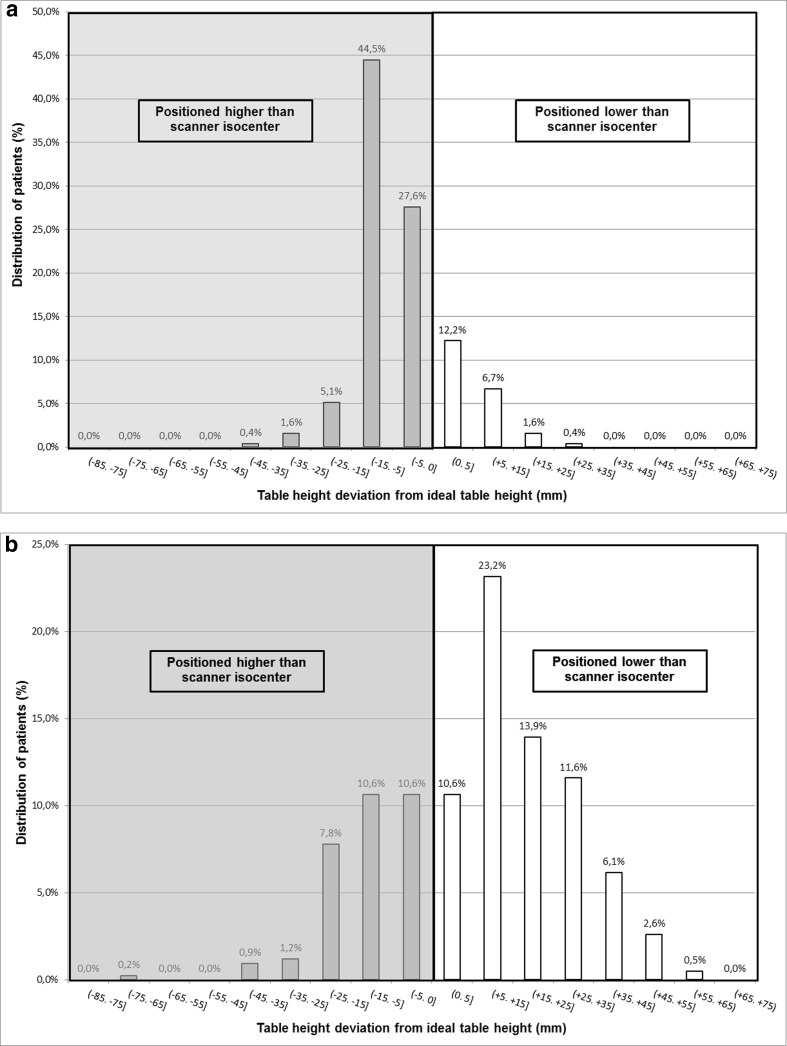
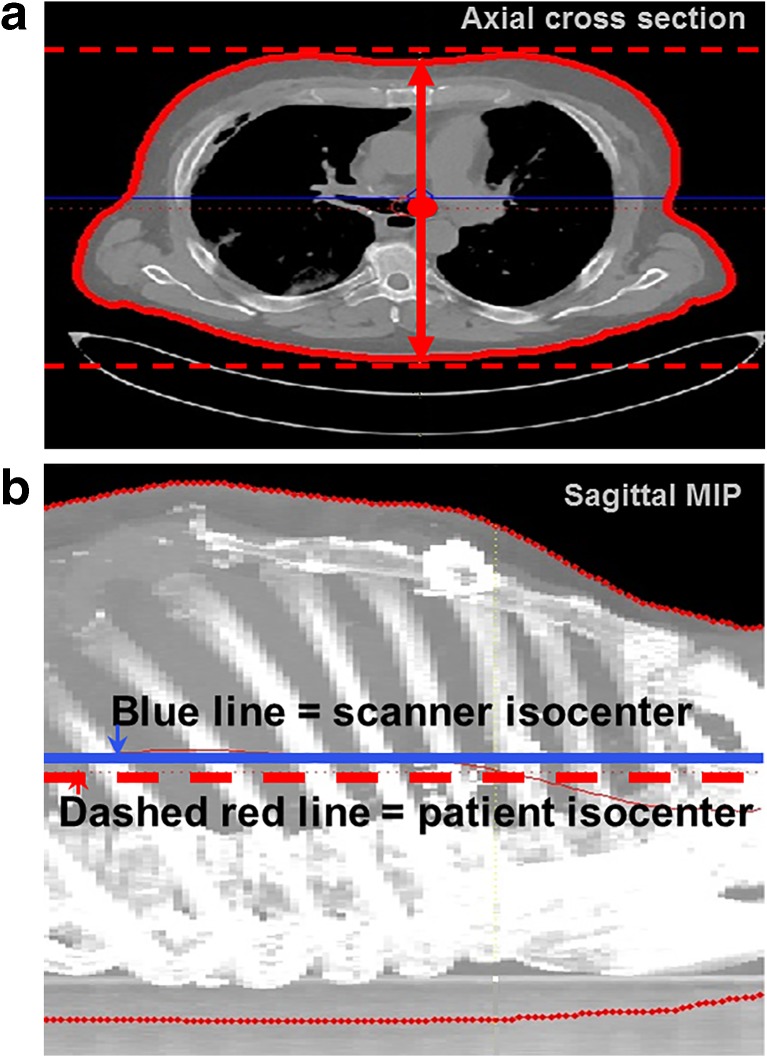
Four hundred twenty-three patients that underwent CT of the head, thorax, and/or abdomen on a scanner with manual table height selection and 254 patients on a scanner with table height suggestion by a 3D camera were retrospectively included. Within the camera group, table height suggestion was based on infrared body contour detection and fitting of a scalable patient model to the 3D data. Proper positioning was defined as the ideal table height at which the scanner isocenter coincides with the patient's isocenter. Patient isocenter was computed by automatic skin contour extraction in each axial image and averaged over all images. Table heights suggested by the camera and selected by the radiographer were compared with the ideal height.
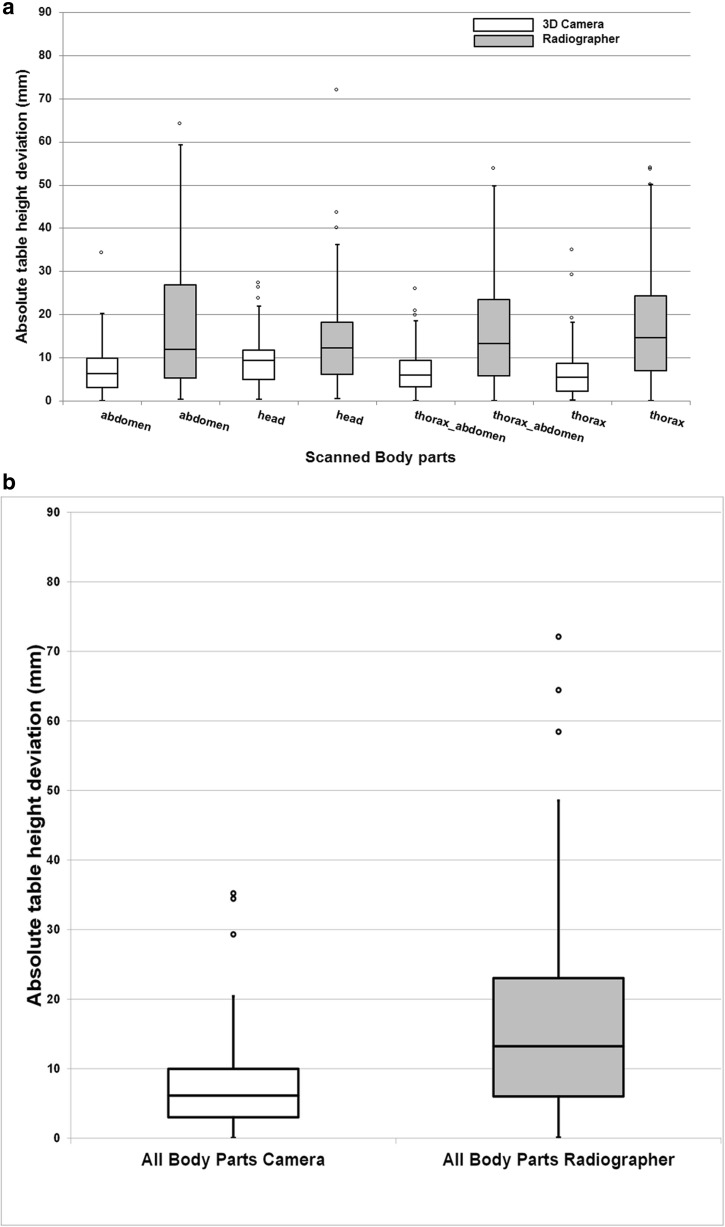
Median (interquartile range) absolute table height deviation in millimeter was 12.0 (21.6) for abdomen, 12.2 (12.0) for head, 13.4 (17.6) for thorax-abdomen, and 14.7 (17.3) for thorax CT scans positioned by radiographers. The deviation was significantly less (p < 0.01) for the 3D camera at 6.3 (6.9) for abdomen, 9.5 (6.8) for head, 6.0 (6.1) for thorax-abdomen, and 5.4 (6.4) mm for thorax.
A 3D camera for body contour detection allows for accurate patient positioning, thereby outperforming manual positioning done by radiographers, resulting in significantly smaller deviations from the ideal table height. However, radiographers remain indispensable when the system fails or in challenging cases.
• A 3D camera for body contour detection allows for accurate patient positioning. • A 3D camera outperformed radiographers in patient positioning in CT. • Deviation from ideal table height was more extreme for patients positioned by radiographers for all body parts.
评估 3D 相机在 CT 中进行身体轮廓检测和患者定位的准确性,与放射技师的常规手动定位相比。
回顾性纳入 423 例头部、胸部和/或腹部行手动选择床高 CT 扫描的患者和 254 例行 3D 相机提示床高 CT 扫描的患者。在相机组中,床高提示基于红外身体轮廓检测和可缩放患者模型与 3D 数据的拟合。适当的定位定义为使扫描仪等中心与患者等中心重合的理想床高。患者等中心通过在每个轴向图像中自动提取皮肤轮廓并在所有图像上平均计算得出。相机提示的床高和放射技师选择的床高与理想高度进行比较。
腹部、头部、胸腹部和胸部 CT 扫描的放射技师定位的平均(四分位距)绝对床高偏差分别为 12.0(21.6)mm、12.2(12.0)mm、13.4(17.6)mm 和 14.7(17.3)mm。使用 3D 相机时,偏差显著减小(p < 0.01),分别为腹部 6.3(6.9)mm、头部 9.5(6.8)mm、胸腹部 6.0(6.1)mm 和胸部 5.4(6.4)mm。
身体轮廓检测的 3D 相机可实现患者的精确定位,优于放射技师的手动定位,从而使与理想床高的偏差显著减小。然而,在系统故障或在复杂情况下,放射技师仍然不可或缺。
身体轮廓检测的 3D 相机可实现患者的精确定位。
3D 相机在 CT 中患者定位方面优于放射技师。
对于所有身体部位的患者,放射技师定位的患者与理想床高的偏差更大。