Cao Junguo, Lei Ting, Chen Fan, Zhang Chaochao, Ma Chengyuan, Huang Haiyan
Departments of Neurosurgery, First Hospital of Jilin University, Changchun, China.
Neurovascular Research Laboratory and Neurology Department, Vall d'Hebron Research Institute, Universitat Autonoma de Barcelona, Barcelona, Spain.
Medicine (Baltimore). 2018 Oct;97(42):e12703. doi: 10.1097/MD.0000000000012703.
A sellar mass in children is most often seen in craniopharyngeal tumors, intracranial germ cell tumors, or pituitary adenomas. However, pituitary hyperplasia secondary to primary hypothyroidism (PHPH) is not commonly seen in children.
A 10-year-old girl was admitted due to growth retardation and obesity for 4 years. On physical examination, the patient had a height of 118 cm, body weight of 46 kg, body mass index (BMI) of 33.0 kg/m.
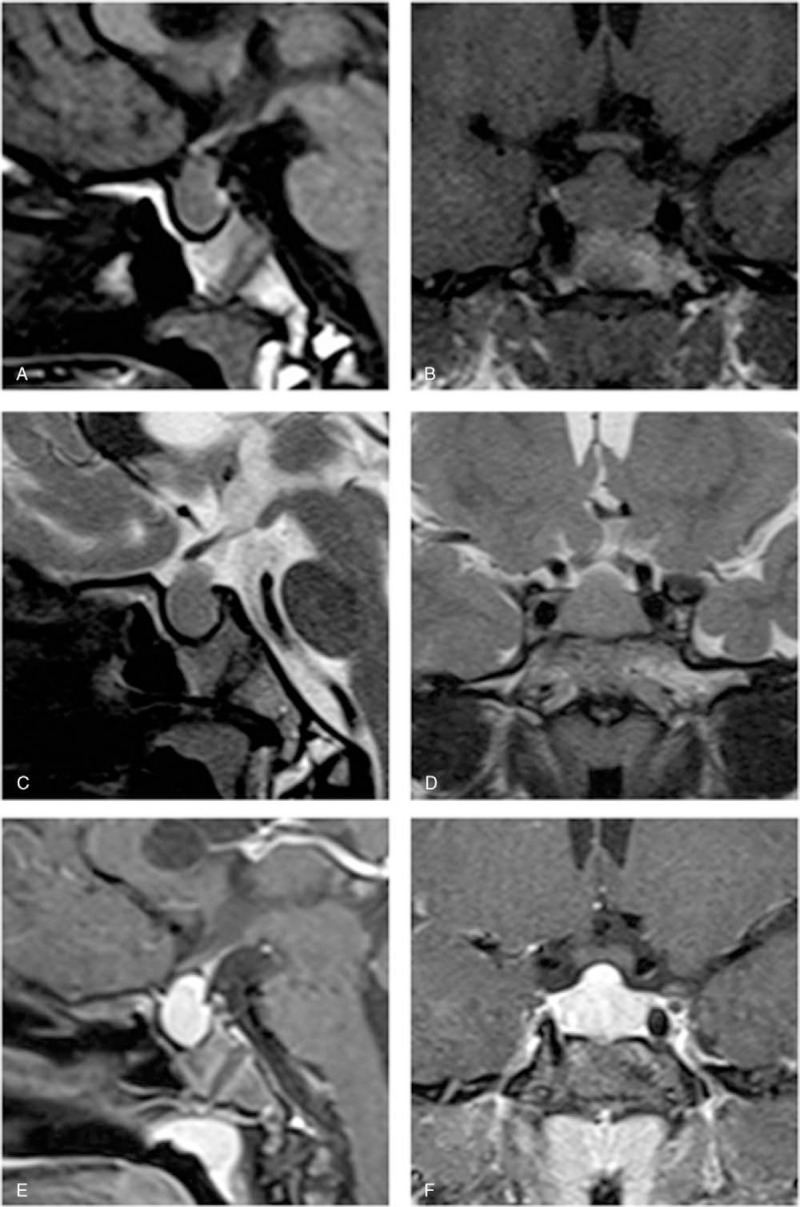
After magnetic resonance imaging (MRI) and laboratory tests, her initial diagnosis was Hashimoto's thyroiditis, primary hypothyroidism, and reactive pituitary hyperplasia.
She was treated with oral L-thyroxine tablets.
After 6 months, physical examination showed a height of 125 cm, weight of 36 kg, BMI of 23.0 kg/m. She developed well, with 12 cm of yearly growth thereafter.
The diagnosis of PHPH in a child is very important and sometimes difficult. Based on the summary and analysis of previous cases, we can learn that the main manifestations of PHPH include growth arrest and obesity, perhaps accompanied by symptoms caused by a decreased thyroid hormone concentration and elevated prolactin (PRL) concentration. Intracranial MRI shows diffuse enlargement of the anterior lobe of the pituitary gland, with a dome-shaped blunt edge change. Thyroid hormone levels may decrease, whereas the thyroid stimulating hormone (TSH) level increases, commonly accompanied by an elevated PRL, reduced growth hormone (GH) levels, and positive findings of TPOAb and TGAb. Improvement of symptoms and the normalization of hormone levels as well as restoration of pituitary size can be achieved after treated with thyroid hormone replacement therapy. And a hasty decision on surgical resection should be avoided when the diagnosis is uncertain.
儿童鞍区肿块最常见于颅咽管瘤、颅内生殖细胞瘤或垂体腺瘤。然而,原发性甲状腺功能减退继发的垂体增生(PHPH)在儿童中并不常见。
一名10岁女孩因生长发育迟缓及肥胖4年入院。体格检查显示,患者身高118厘米,体重46千克,体重指数(BMI)为33.0千克/平方米。
经磁共振成像(MRI)及实验室检查,其初步诊断为桥本甲状腺炎、原发性甲状腺功能减退及反应性垂体增生。
给予口服左甲状腺素片治疗。
6个月后,体格检查显示身高125厘米,体重36千克,BMI为23.0千克/平方米。她发育良好,此后每年生长12厘米。
儿童PHPH的诊断非常重要且有时颇具难度。通过对既往病例的总结分析可知,PHPH的主要表现包括生长停滞和肥胖,可能伴有甲状腺激素浓度降低及催乳素(PRL)浓度升高所致的症状。颅内MRI显示垂体前叶弥漫性增大,边缘呈圆顶状钝性改变。甲状腺激素水平可能降低,而促甲状腺激素(TSH)水平升高,常伴有PRL升高、生长激素(GH)水平降低以及甲状腺过氧化物酶抗体(TPOAb)和甲状腺球蛋白抗体(TGAb)阳性。经甲状腺激素替代治疗后,症状可改善,激素水平恢复正常,垂体大小也可恢复。诊断不明确时应避免仓促决定手术切除。