School of Public Health, Faculty of Health Sciences, University of the Witwatersrand, Parktown, Johannesburg, South Africa.
Dodowa Health Research Centre, Dodowa, Ghana.
PLoS One. 2018 Oct 22;13(10):e0205370. doi: 10.1371/journal.pone.0205370. eCollection 2018.
Maternal mortality was the subject of the United Nations' fifth Millennium Development Goal which was to reduce the maternal mortality ratio by three quarters from 1990 to 2015. The Sustainable Development Goals (SDGs), target 3.1 requires participating countries to reduce their maternal mortality ratio to less than 70 deaths per 100,000 live births by 2030. Although much research has been conducted, knowing the spatial patterns and risk factors associated with maternal mortality in developing countries helps target scarce resources and intervention programmes to high risk areas for the greatest impact.
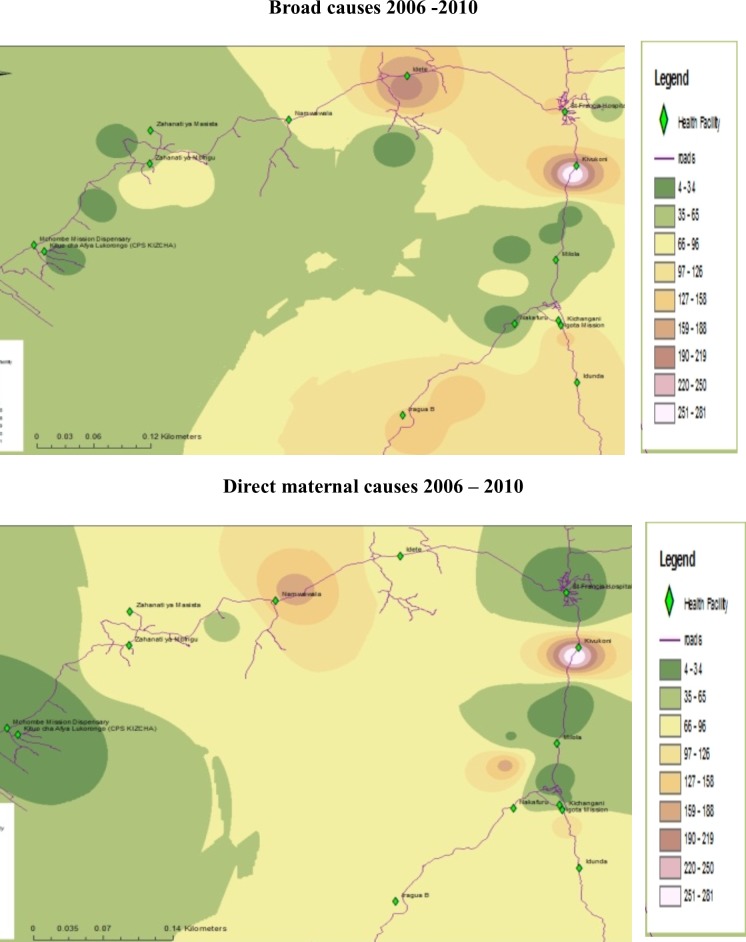
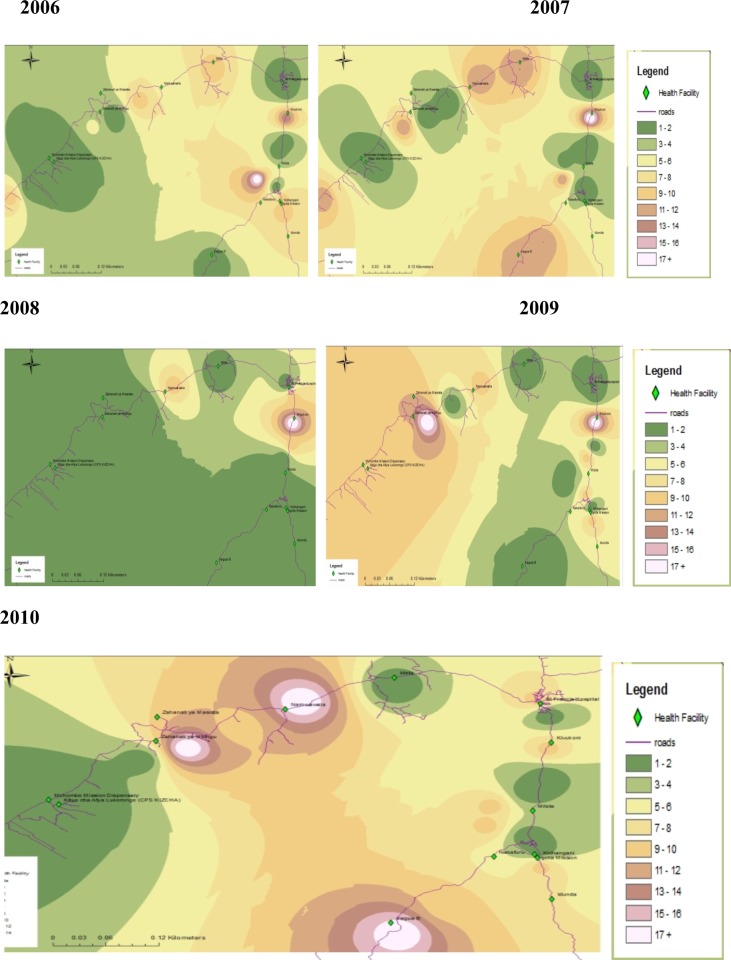
Data were analysed from a longitudinal open cohort of women aged 15 to 49 years, enrolled from 2006 to 2010. An inverse distance weighted method of interpolation was used to assess spatial patterns of maternal mortality. Cox proportional hazards regression analysis was used to identify risk factors associated with maternal mortality.
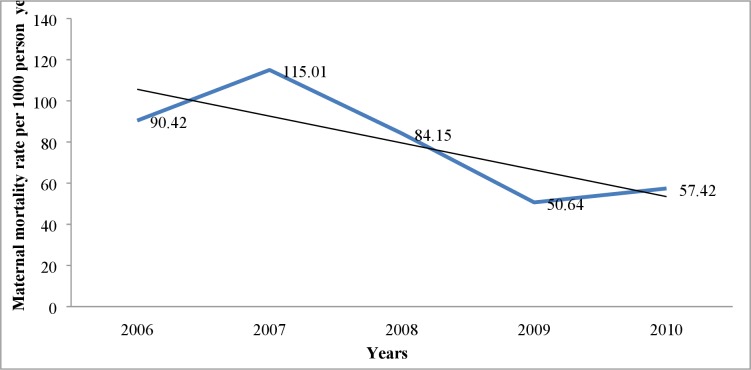
The overall maternal mortality rate for the 36 792 study participants for the five years was 0.79 per 1000 person years. The trend declined from 90.42 in 2006 to 57.42 in 2010. Marked geographical differences were observed in maternal mortality patterns. The main causes of maternal death were eclampsia (23%), haemorrhage (22%) and abortion-related complications (10%). There was a reduced risk of 82% (HR = 0.18, 95% CI:0.05-0.74) and 78% (HR = 0.22, 95% CI:0.05-0.92) for women aged 20-29 and 30-39 years, respectively, compared with those younger than 20 years. While being married had a protective effect of 94% (HR = 0.06, 95% CI: 0.01-0.51) compared with being single, women who were widowed had an increased risk of maternal death of 913% (HR = 9.13, 95% CI: 1.02-81.94). Women who belong to poorer, poor and least poor socioeconomic quintile had 84%, 71% and 72% reduction in risk of maternal mortality respectively compared to those in the poorest category (HR = 0.16, 95% CI: 0.06-0.42; HR = 0.29, 95% CI: 0.12-0.69; HR = 0.28, 95% CI: 0.10-0.80).
Maternal mortality has declined in rural southern Tanzania since 2006, with geographical differences in patterns of death. Eclampsia, haemorrhage and abortion-related complications are the three leading causes of maternal death in the region, with risk factors being younger than 20 years, being single or widowed, and having a low socioeconomic status.
孕产妇死亡率是联合国第五个千年发展目标的主题,该目标旨在将 1990 年至 2015 年的孕产妇死亡率降低四分之三。可持续发展目标(SDGs)目标 3.1 要求参与国将其孕产妇死亡率降低到每 10 万例活产中少于 70 例,到 2030 年。尽管已经进行了大量研究,但了解发展中国家孕产妇死亡率的空间模式和相关风险因素有助于将稀缺资源和干预计划瞄准高风险地区,以产生最大影响。
对 2006 年至 2010 年期间招募的年龄在 15 至 49 岁的女性进行了一项纵向开放式队列研究的数据进行了分析。使用逆距离加权插值方法评估孕产妇死亡率的空间模式。使用 Cox 比例风险回归分析确定与孕产妇死亡率相关的风险因素。
在五年期间,36792 名研究参与者的总体孕产妇死亡率为每 1000 人年 0.79 人。趋势从 2006 年的 90.42 人下降到 2010 年的 57.42 人。在孕产妇死亡率模式方面观察到明显的地域差异。孕产妇死亡的主要原因是子痫(23%)、出血(22%)和与流产相关的并发症(10%)。与 20 岁以下的女性相比,20-29 岁和 30-39 岁的女性的死亡风险分别降低了 82%(HR = 0.18,95%CI:0.05-0.74)和 78%(HR = 0.22,95%CI:0.05-0.92)。与单身相比,已婚女性的死亡风险降低了 94%(HR = 0.06,95%CI:0.01-0.51),而丧偶女性的死亡风险增加了 913%(HR = 9.13,95%CI:1.02-81.94)。与最贫困的类别相比,属于较贫穷、贫穷和最不贫穷社会经济五分位数的女性的孕产妇死亡率风险分别降低了 84%、71%和 72%(HR = 0.16,95%CI:0.06-0.42;HR = 0.29,95%CI:0.12-0.69;HR = 0.28,95%CI:0.10-0.80)。
自 2006 年以来,坦桑尼亚南部农村地区的孕产妇死亡率有所下降,死亡模式存在地域差异。子痫、出血和与流产相关的并发症是该地区孕产妇死亡的三个主要原因,风险因素是 20 岁以下、单身或丧偶以及社会经济地位较低。