Department of Anaesthesiology, General Intensive Care and Pain Medicine, Medical University of Vienna, Waehringer Gürtel 18-20, A-1090, Vienna, Austria.
RAIC Laboratory 13C1, Medical University of Vienna, Waehringer Gürtel 18-20, A-1090, Vienna, Austria.
Crit Care. 2018 Oct 26;22(1):267. doi: 10.1186/s13054-018-2198-3.
The continuous administration of opioids in critical care patients is a common therapy for the tolerance of mechanical ventilation. Opioid choice has a crucial impact on the length of mechanical ventilation. Owing to its very short context-sensitive half-life, remifentanil widens the available options for sedoanalgetic strategies. Supply disruption of such established intensive care medication has been reported to worsen clinical outcomes.
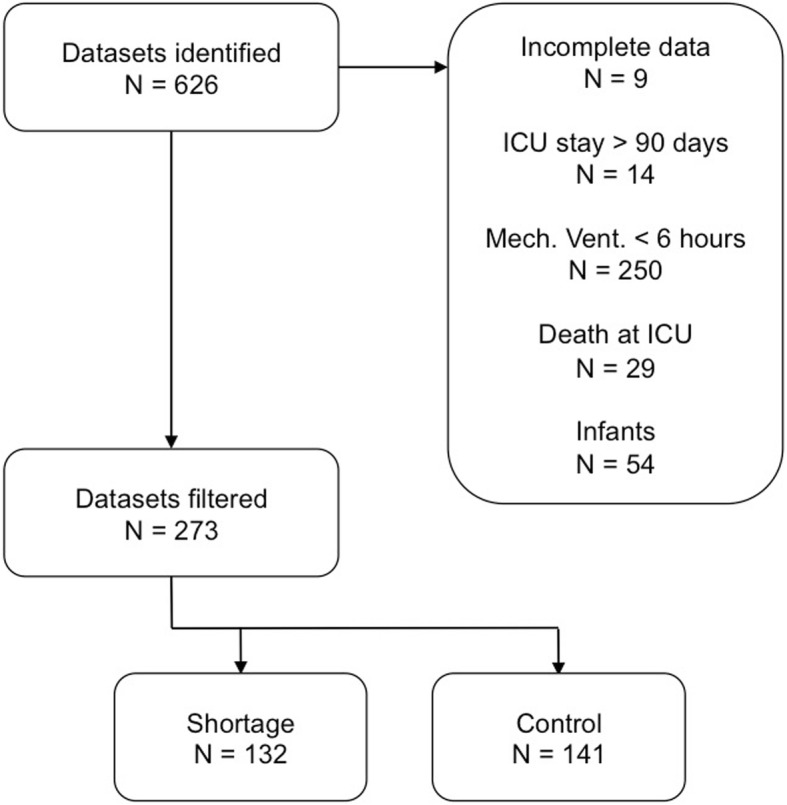
This retrospective study investigated the influence of a nationwide supply shortage of remifentanil on mechanical ventilation and ventilation-associated outcomes at three perioperative intensive care units (ICUs) in a tertiary care hospital in Vienna. Two groups were followed: patients admitted to the ICU during the remifentanil shortage (July 1, 2016 to September 30, 2016) and a control group one year after the remifentanil shortage (July 1, 2017 to September 30, 2017). Included patients were adults, received mechanical ventilation for at least 6 h, were admitted less than 90 days in the respective ICU, and survived their admission.
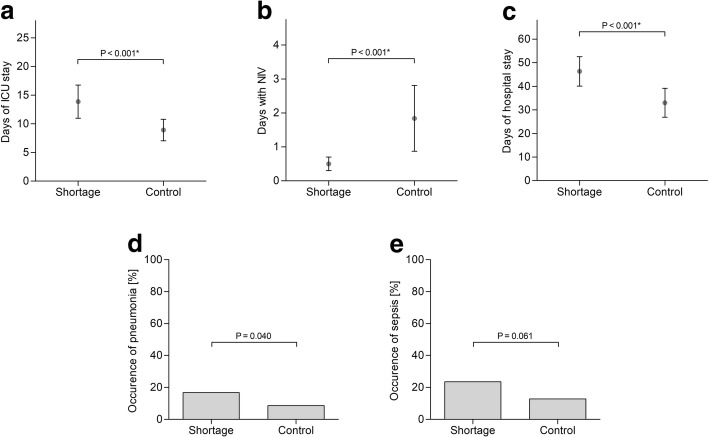
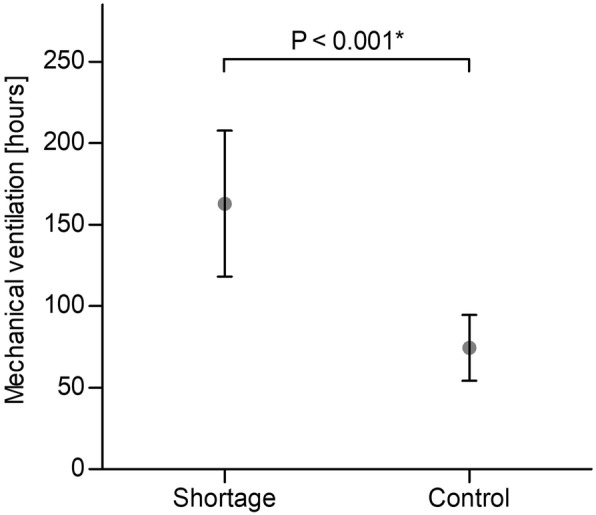
For comparison, Poisson count regression models and logistic regression models were computed. To compensate for multiple testing, the significance level was split (0.02 for the primary and 0.006 for secondary outcome parameters). Patients in the remifentanil shortage group received significantly longer mechanical ventilation (risk ratio 2.19, 95% confidence interval 2.14-2.24, P <0.001) with significantly prolonged ICU stay (P <0.001), days with non-invasive ventilation (P <0.001), and length of hospital stay (P <0.001). No significant difference was found in the occurrence of pneumonia (P = 0.040) and sepsis (P = 0.061). A greater proportion of patients in the shortage group underwent secondary tracheostomy (P <0.001).
The remifentanil shortage caused a significant impairment of essential outcome parameters in the ICU.
在重症监护患者中持续给予阿片类药物是机械通气耐受的常见治疗方法。阿片类药物的选择对机械通气的时间长短有至关重要的影响。由于其非常短的上下文敏感半衰期,瑞芬太尼为镇静镇痛策略提供了更多选择。据报道,此类既定重症监护药物的供应中断会使临床结果恶化。
本回顾性研究调查了维也纳一家三级护理医院的三个围手术期重症监护病房(ICU)中全国范围内瑞芬太尼供应短缺对机械通气和与通气相关的结果的影响。随访了两组患者:在瑞芬太尼短缺期间(2016 年 7 月 1 日至 9 月 30 日)入住 ICU 的患者和瑞芬太尼短缺一年后(2017 年 7 月 1 日至 9 月 30 日)入住 ICU 的对照组患者。纳入标准为成人、至少接受 6 小时机械通气、入住 ICU 时间不到 90 天且存活出院。
为了进行比较,计算了泊松计数回归模型和逻辑回归模型。为了补偿多次检验,将显著性水平分割(主要结果参数为 0.02,次要结果参数为 0.006)。瑞芬太尼短缺组患者接受机械通气的时间明显延长(风险比 2.19,95%置信区间 2.14-2.24,P<0.001),ICU 入住时间(P<0.001)、无创通气天数(P<0.001)和住院时间(P<0.001)均延长。肺炎(P=0.040)和脓毒症(P=0.061)的发生率无显著差异。短缺组中接受二次气管切开术的患者比例显著更高(P<0.001)。
瑞芬太尼短缺显著损害了 ICU 的重要结局参数。