Neyra Javier A, Mescia Federica, Li Xilong, Adams-Huet Beverley, Yessayan Lenar, Yee Jerry, Toto Robert D, Moe Orson W
Division of Nephrology, Bone and Mineral Metabolism, Department of Internal Medicine, University of Kentucky, Lexington, Kentucky, USA.
Charles and Jane Pak Center for Mineral Metabolism and Clinical Research, University of Texas Southwestern Medical Center, Dallas, Texas, USA.
Kidney Int Rep. 2018 Jul 29;3(6):1344-1353. doi: 10.1016/j.ekir.2018.07.016. eCollection 2018 Nov.
Chronic kidney disease (CKD) and acute kidney injury (AKI) are strongly associated with excess morbidity and mortality and frequently co-occur in critically ill septic patients, but how their interplay affects clinical outcomes is not well elucidated.
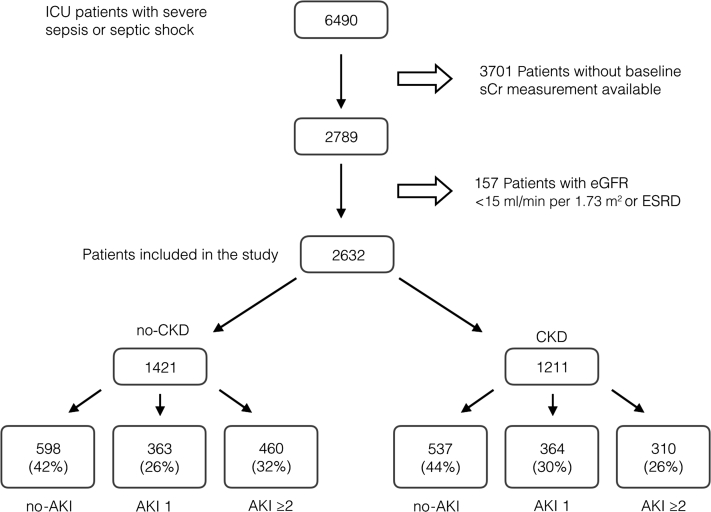
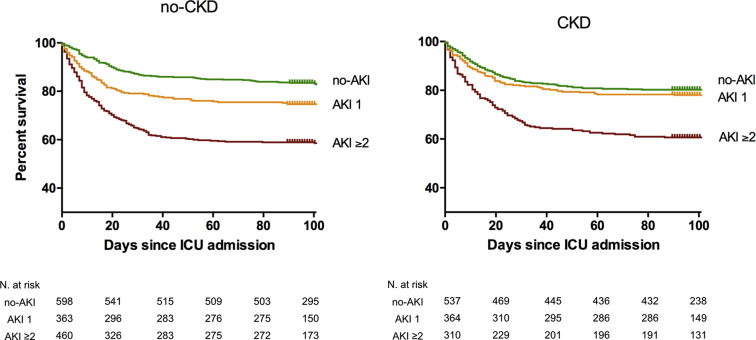
We conducted a single-center, retrospective cohort study of 2632 adult patients admitted to the intensive care unit (ICU) with severe sepsis or septic shock. Subjects were classified into 6 groups according to baseline CKD (no-CKD: estimated glomerular filtration rate [eGFR] ≥60; CKD: eGFR 15-59 ml/min per 1.73 m) and incident AKI by the Kidney Disease: Improving Global Outcomes (KDIGO) serum creatinine criteria (no-AKI, AKI stage 1, AKI stages ≥2) during ICU stay. Study outcomes were 90-day mortality (in hospital or within 90 days of discharge) and incident/progressive CKD.
Prevalent CKD was 46% and incident AKI was 57%. Adjusted hazard ratios (95% confidence intervals) for 90-day mortality relative to the reference group of no-CKD/no-AKI were 1.5 (1.1-2.0) in no-CKD/AKI stage 1, 2.4 (1.9-3.1) in no-CKD/AKI stages≥2, 1.1 (0.8-1.4) in CKD/no-AKI, 1.2 (0.9-1.6) in CKD/AKI stage 1, and 2.2 (1.7-2.9) in CKD/AKI stages ≥2. A similar trend was observed for incident/progressive CKD during a median follow-up of 15.3 months.
Stage 1 AKI on CKD was not associated with an independent increased risk of adverse outcomes in critically ill septic patients. AKI stages ≥2 on CKD and any level of AKI in no-CKD patients were strongly and independently associated with adverse outcomes. Sepsis-associated stage 1 AKI on CKD may represent distinct underlying pathophysiology, with more prerenal cases and less severe intrinsic damage, which needs further investigation.
慢性肾脏病(CKD)和急性肾损伤(AKI)与发病率和死亡率过高密切相关,且在重症脓毒症患者中经常同时出现,但它们之间的相互作用如何影响临床结局尚未得到充分阐明。
我们对2632名因严重脓毒症或脓毒性休克入住重症监护病房(ICU)的成年患者进行了一项单中心回顾性队列研究。根据基线CKD(无CKD:估计肾小球滤过率[eGFR]≥60;CKD:eGFR 15 - 59 ml/min/1.73 m²)和ICU住院期间根据肾脏病改善全球预后(KDIGO)血清肌酐标准确定的新发AKI(无AKI、AKI 1期、AKI≥2期)将受试者分为6组。研究结局为90天死亡率(住院期间或出院后90天内)以及新发/进展性CKD。
CKD患病率为46%,新发AKI为57%。相对于无CKD/无AKI的参照组,90天死亡率的校正风险比(95%置信区间)在无CKD/AKI 1期为1.5(1.1 - 2.0),在无CKD/AKI≥2期为2.4(1.9 - 3.1),在CKD/无AKI为1.1(0.8 - 1.4),在CKD/AKI 1期为1.2(0.9 - 1.6),在CKD/AKI≥2期为2.2(1.7 - 2.9)。在中位随访15.3个月期间,新发/进展性CKD也观察到类似趋势。
CKD基础上的1期AKI与重症脓毒症患者不良结局的独立风险增加无关。CKD基础上的AKI≥2期以及无CKD患者的任何程度AKI均与不良结局密切且独立相关。脓毒症相关的CKD基础上的1期AKI可能代表不同的潜在病理生理学,肾前性病例更多且固有损伤较轻,这需要进一步研究。