Mremi Irene R, Rumisha Susan F, Chiduo Mercy G, Mangu Chacha D, Mkwashapi Denna M, Kishamawe Coleman, Lyimo Emanuel P, Massawe Isolide S, Matemba Lucas E, Bwana Veneranda M, Mboera Leonard E G
National Institute for Medical Research, Headquarters, P.O. Box 9653, 11101, Dar es Salaam, Tanzania.
Southern African Centre for Infectious Disease Surveillance, Centre of Excellence for Infectious Diseases of Humans and Animals, P.O. Box 3297, Morogoro, Tanzania.
Popul Health Metr. 2018 Nov 20;16(1):16. doi: 10.1186/s12963-018-0175-3.
Accurate and reliable hospital information on the pattern and causes of death is important to monitor and evaluate the effectiveness of health policies and programs. The objective of this study was to assess the availability, accessibility, and quality of hospital mortality data in Tanzania.
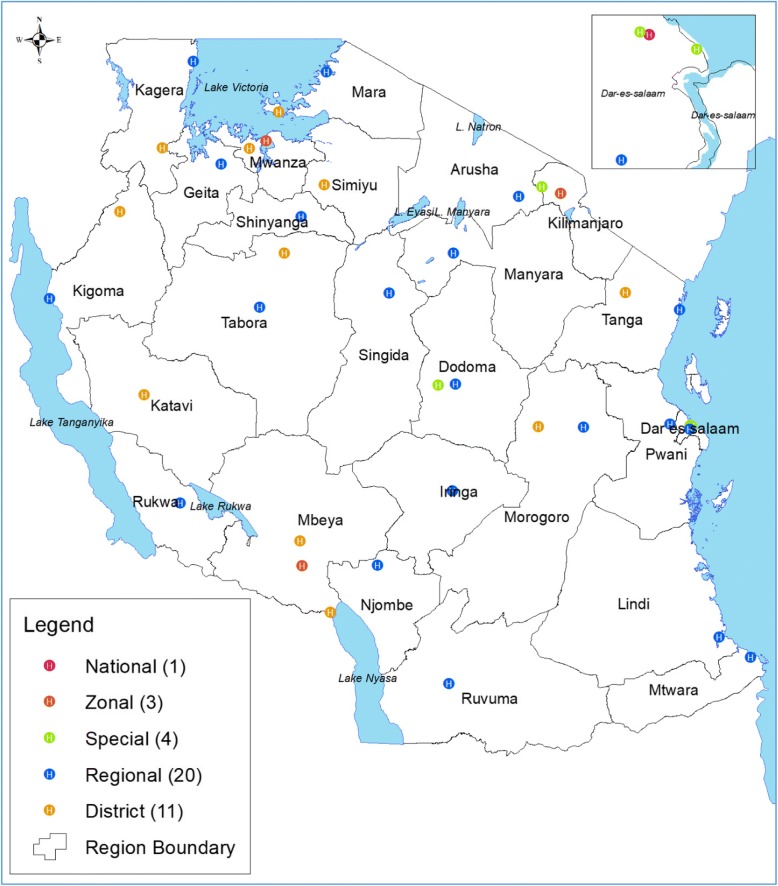
This cross-sectional study involved selected hospitals of Tanzania and was carried out from July to October 2016. Review of hospital death registers and forms was carried out to cover a period of 10 years (2006-2015). Interviews with hospital staff were conducted to seek information as regards to tools used to record mortality data, staff involved in recording and availability of data storage and archiving facilities.
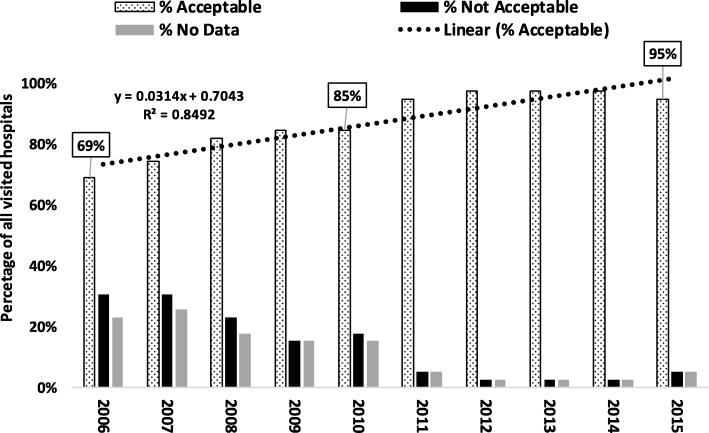
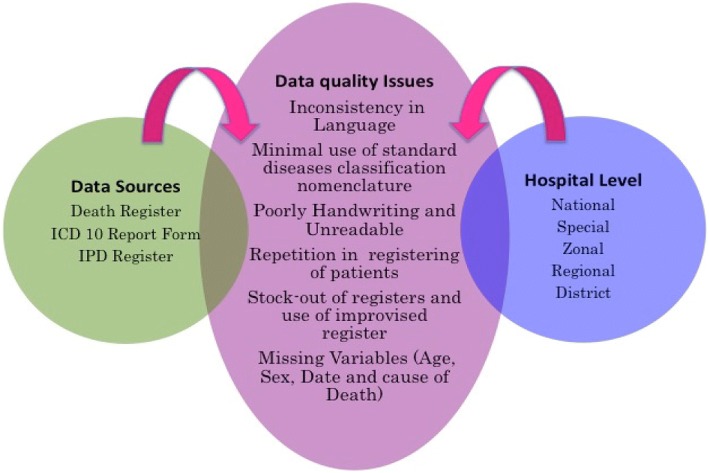
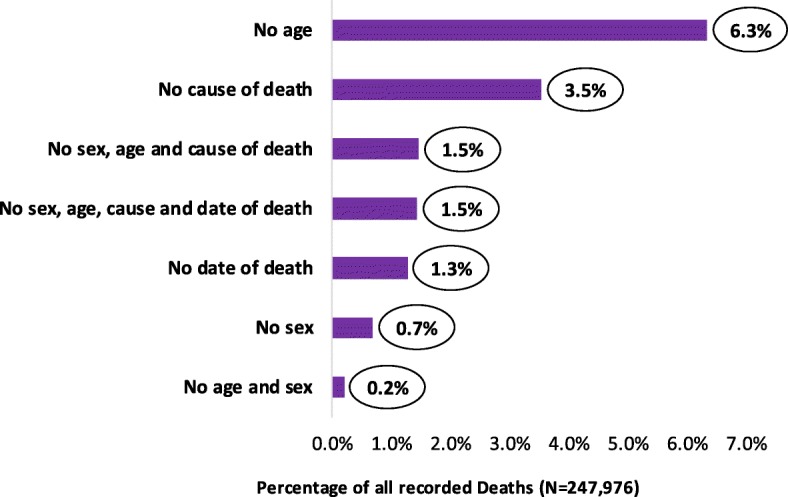
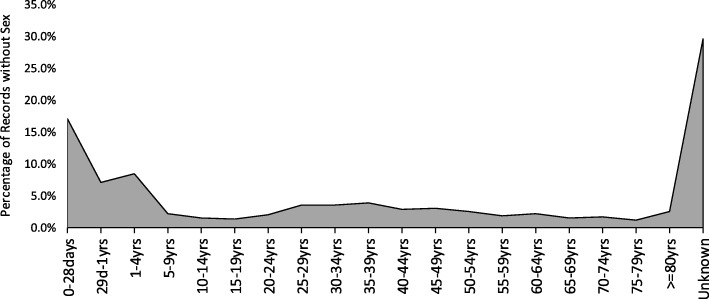
A total of 247,976 death records were reviewed. The death register was the most (92.3%) common source of mortality data. Other sources included the International Classification of Diseases (ICD) report forms, Inpatient registers, and hospital administrative reports. Death registers were available throughout the 10-year period while ICD-10 forms were available for the period of 2013-2015. In the years between 2006 and 2010 and 2011-2015, the use of death register increased from 82 to 94.9%. Three years after the introduction of ICD-10 procedure, the forms were available and used in 28% (11/39) hospitals. The level of acceptable data increased from 69% in 2006 to 97% in 2015. Inconsistency in the language used, use of non-standard nomenclature for causes of death, use of abbreviations, poorly and unreadable handwriting, and missing variables were common data quality challenges. About 6.3% (n = 15,719) of the records had no patient age, 3.5% (n = 8790) had no cause of death and ~ 1% had no sex indicated. The frequency of missing sex variable was most common among under-5 children. Data storage and archiving in most hospitals was generally poor. Registers and forms were stored in several different locations, making accessibility difficult.
Overall, this study demonstrates gaps in hospital mortality data availability, accessibility, and quality, and highlights the need for capacity strengthening in data management and periodic record reviews. Policy guidelines on the data management including archiving are necessary to improve data.
准确可靠的医院死亡模式及原因信息对于监测和评估卫生政策与项目的有效性至关重要。本研究的目的是评估坦桑尼亚医院死亡率数据的可得性、可及性和质量。
这项横断面研究涉及坦桑尼亚选定的医院,于2016年7月至10月开展。对医院死亡登记册和表格进行审查,涵盖10年期间(2006 - 2015年)。与医院工作人员进行访谈,以获取有关记录死亡率数据所使用工具、参与记录的人员以及数据存储和存档设施可用性的信息。
共审查了247,976份死亡记录。死亡登记册是最常见(92.3%)的死亡率数据来源。其他来源包括国际疾病分类(ICD)报告表格、住院患者登记册和医院行政报告。死亡登记册在整个10年期间都有,而ICD - 10表格在2013 - 2015年期间可用。在2006年至2010年以及2011年至2015年期间,死亡登记册的使用从82%增加到94.9%。引入ICD - 10程序三年后,这些表格在28%(11/39)的医院中可用并得到使用。可接受数据的水平从2006年的69%提高到2015年的97%。语言使用不一致、死因使用非标准术语、使用缩写、字迹潦草难以辨认以及变量缺失是常见的数据质量挑战。约6.3%(n = 15,719)的记录没有患者年龄,3.5%(n = 8790)没有死因,约1%未注明性别。性别变量缺失的频率在5岁以下儿童中最为常见。大多数医院的数据存储和存档普遍较差。登记册和表格存放在几个不同的地方,难以获取。
总体而言,本研究表明医院死亡率数据在可得性、可及性和质量方面存在差距,并强调了加强数据管理能力和定期记录审查的必要性。关于包括存档在内的数据管理的政策指南对于改善数据是必要的。