Zellweger Ueli, Junker Christoph, Bopp Matthias
Epidemiology, Biostatistics and Prevention Institute, University of Zurich, Hirschengraben 84, CH-8001, Zürich, Switzerland.
Swiss Federal Statistical Office, Espace de l'Europe 10, 2010, Neuchâtel, Switzerland.
Popul Health Metr. 2019 Mar 1;17(1):2. doi: 10.1186/s12963-019-0182-z.
Cause of death statistics are an important tool for quality control of the health care system. Their reliability, however, is controversial. Comparing death certificates with their corresponding medical records is implemented only occasionally but may point to quality problems. We aimed at exploring the agreement between information in the cause of death statistics and hospital discharge diagnoses at death.
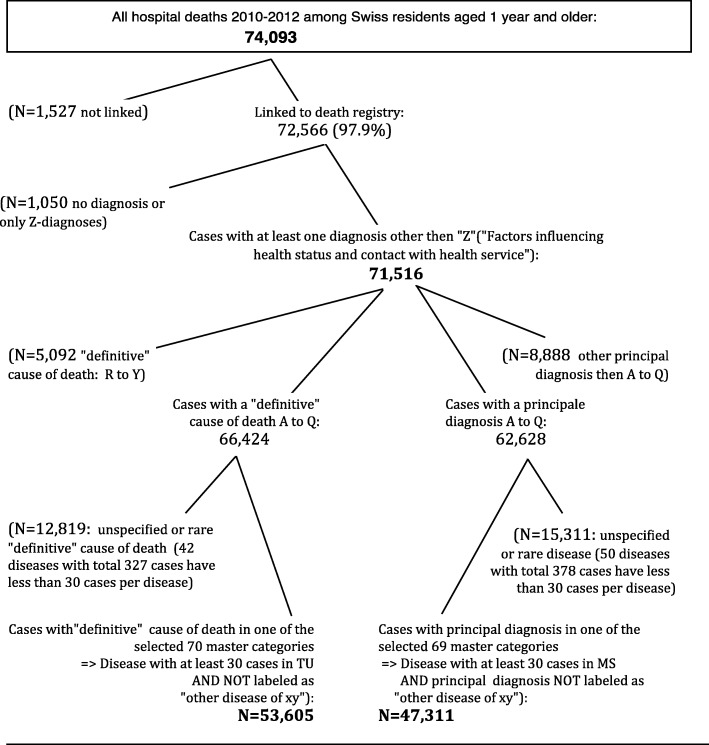
Selection of disease categories was based on ICD-10 Tabulation List for Morbidity and ICD-10 Mortality Tabulation List 2. Index cases were defined as deaths having occurred among Swiss residents 2010-2012 in a hospital and successfully linked to the Swiss National Cohort. Rare, external and ill-defined causes were excluded from comparison, leaving 53,605 deaths from vital statistics and 47,311 deaths from hospital discharge statistics. For 95% of individuals, respective information from the 2000 census could be retrieved and used for multiple logistic regression.
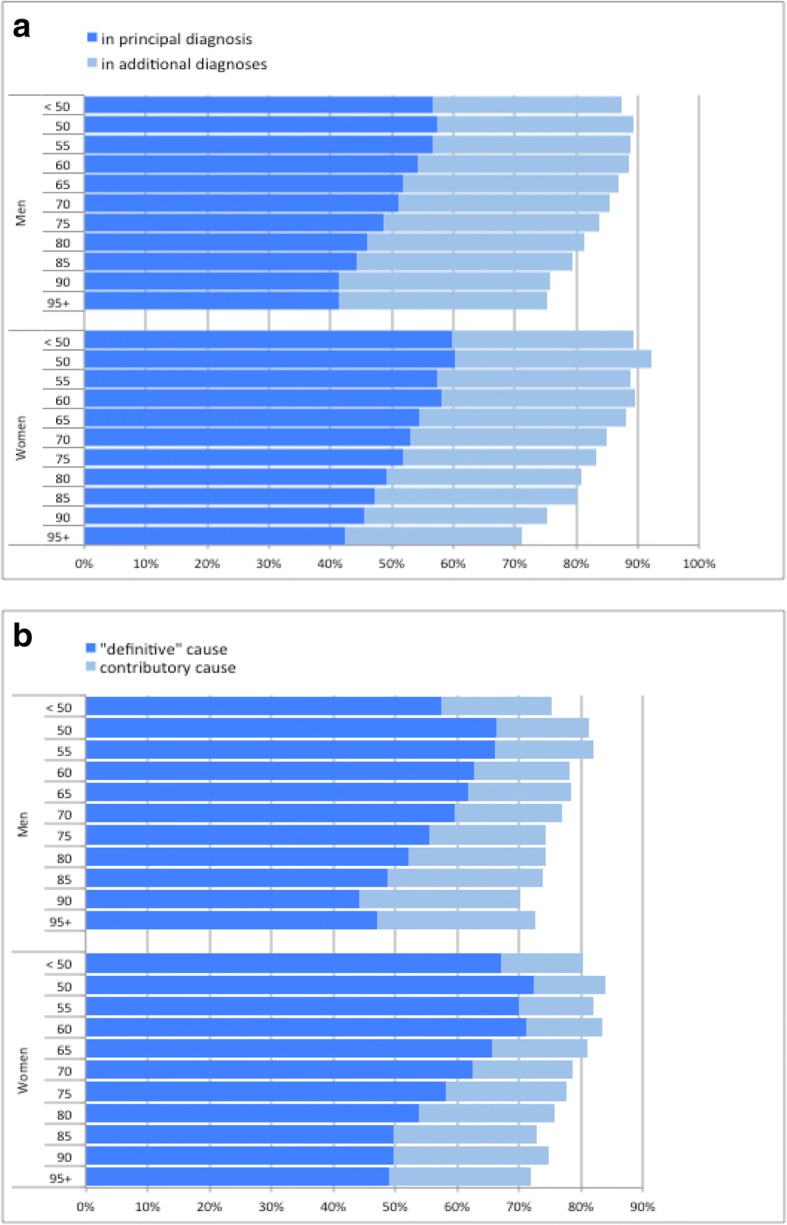
For 83% of individuals the underlying cause of death could be traced among hospital diagnoses and for 77% the principal hospital diagnosis among the cause of death information. Mirroring different evaluation of complex situations by individual physicians, rates of agreement varied widely depending on disease/cause of death, but were generally in line with similar studies. Multiple logistic regression revealed however significant variation in reporting that could not entirely be explained by age or cause of death of the deceased suggesting differential exploitation of available diagnosis information.
Substantial regional variation and lower agreement rates among socially disadvantaged groups like single, less educated, or culturally less integrated persons suggest potential for improving reporting of diagnoses and causes of death by physicians in Switzerland. Studies of this kind should be regularly conducted as a quality monitoring.
死因统计是医疗保健系统质量控制的重要工具。然而,其可靠性存在争议。将死亡证明与其相应的病历进行比较只是偶尔进行,但可能会指出质量问题。我们旨在探讨死因统计信息与死亡时医院出院诊断之间的一致性。
疾病类别的选择基于《国际疾病分类第10版发病率列表》和《国际疾病分类第10版死亡率列表2》。索引病例定义为2010 - 2012年在瑞士医院发生且成功与瑞士国家队列相关联的瑞士居民死亡病例。罕见、外部和定义不明确的死因被排除在比较之外,留下生命统计中的53,605例死亡病例和医院出院统计中的47,311例死亡病例。对于95%的个体,可以检索到2000年人口普查的相应信息并用于多因素逻辑回归。
对于83%的个体,可在医院诊断中追溯到根本死因,对于77%的个体,可在死因信息中找到主要医院诊断。反映个体医生对复杂情况的不同评估,一致性率因疾病/死因差异很大,但总体上与类似研究一致。然而,多因素逻辑回归显示报告存在显著差异,这不能完全由死者的年龄或死因来解释,表明对可用诊断信息的利用存在差异。
在单身、受教育程度较低或文化融合程度较低等社会弱势群体中存在显著的地区差异和较低的一致性率,这表明瑞士医生在诊断和死因报告方面有改进的潜力。此类研究应定期进行作为质量监测。