Public Health Wales, Cardiff, UK.
Department of Public Health, University of Liverpool, Liverpool, UK.
J Epidemiol Community Health. 2019 Feb;73(2):162-167. doi: 10.1136/jech-2018-211141. Epub 2018 Nov 23.
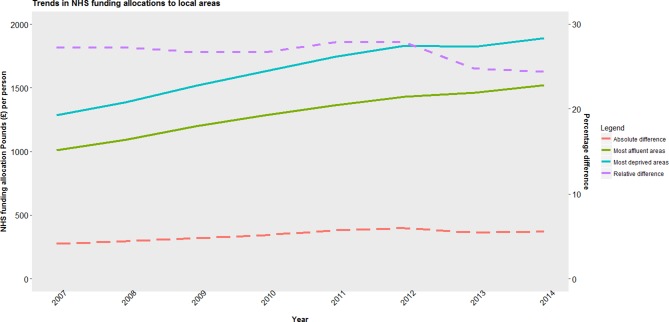
Health investment in England post-2010 has increased at lower rates than previously, with proportionally less being allocated to deprived areas. This study seeks to explore the impact of this on inequalities in amenable mortality between local areas.
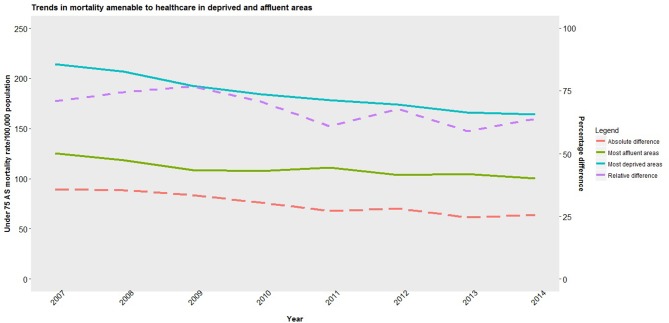
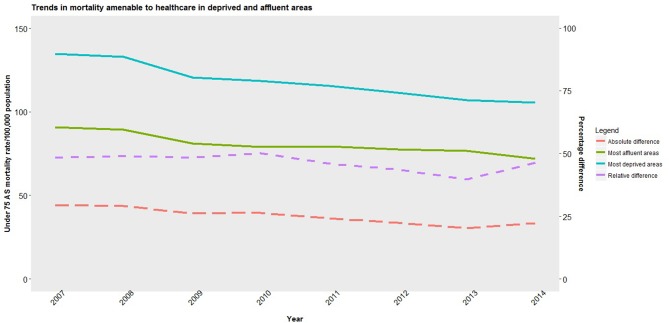
We undertook a time-series analysis across 324 lower-tier local authorities in England, evaluating the impact of changes in funding allocations to health commissioners from 2007 to 2014 on spatial inequalities in age-standardised under-75 mortality rates for conditions amenable to healthcare for men and women, adjusting for trends in household income, unemployment and time-trends.
More deprived areas received proportionally more funding between 2007 and 2014, though the reorganisation of commissioning in 2012 stalled this. Funding increases to more deprived local areas accounted for a statistically significant reduction in inequalities in male amenable mortality between local areas of 13 deaths per 100 000 (95% CI 2.5 to 25.9). Funding changes were associated with a reduction in inequalities in female amenable mortality of 7.0 per 100,000, though this finding did not reach significance (p=0.09).
Current National Health Service (NHS) resource allocation policy in England appears to be contributing to a convergence in health outcomes between affluent and deprived areas. However, careful surveillance is needed to evaluate whether diminished allocations to more deprived areas in recent years and reduced NHS investment as a whole is impacting adversely on inequalities between groups.
2010 年后,英国的卫生投资增长速度低于以往,分配给贫困地区的比例也相应减少。本研究旨在探讨这对各地区可治疗死亡率不平等的影响。
我们对英格兰 324 个低级别地方当局进行了时间序列分析,评估了 2007 年至 2014 年卫生专员资金分配变化对男性和女性可治疗疾病年龄标准化 75 岁以下死亡率空间不平等的影响,调整了家庭收入、失业率和时间趋势的趋势。
2007 年至 2014 年,较贫困地区获得的资金比例更高,尽管 2012 年的招标重组使其停顿。向较贫困地区提供更多资金,导致地区间男性可治疗死亡率不平等减少了 13 人每 10 万(95%CI 2.5 至 25.9),具有统计学意义。资金变化与女性可治疗死亡率不平等减少 7.0 人每 10 万相关,但这一发现没有达到显著性(p=0.09)。
英国国民保健制度(NHS)目前的资源分配政策似乎正在促使富裕和贫困地区的健康结果趋同。然而,需要进行仔细监测,以评估近年来对较贫困地区的分配减少以及整个 NHS 投资减少是否对群体间的不平等产生不利影响。