Mahmood Javed, Shukla Hem D, Soman Sandrine, Samanta Santanu, Singh Prerna, Kamlapurkar Shriya, Saeed Ali, Amin Neha P, Vujaskovic Zeljko
Department of Radiation Oncology, University of Maryland School of Medicine, Baltimore, MD 21201, USA.
Department of Pharmaceutical Sciences, School of Pharmacy, University of Maryland, Baltimore, MD 21201, USA.
Cancers (Basel). 2018 Nov 28;10(12):469. doi: 10.3390/cancers10120469.
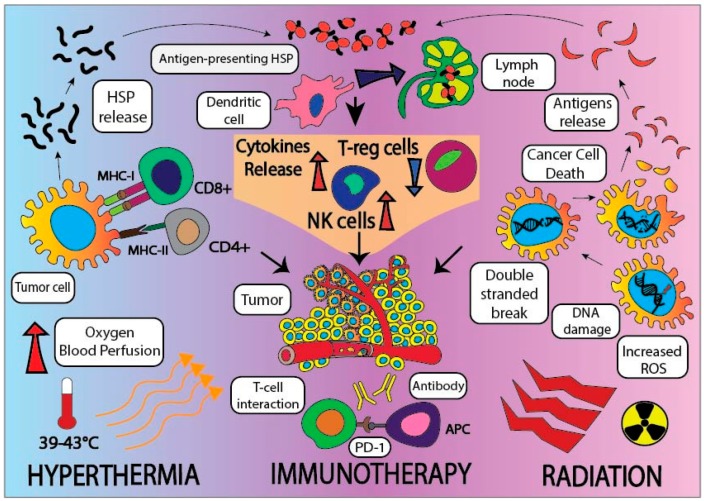
Pancreatic cancer (PC) has the highest mortality rate amongst all other cancers in both men and women, with a one-year relative survival rate of 20%, and a five-year relative survival rate of 8% for all stages of PC combined. The Whipple procedure, or pancreaticoduodenectomy, can increase survival for patients with resectable PC, however, less than 20% of patients are candidates for surgery at time of presentation. Most of the patients are diagnosed with advanced PC, often with regional and distant metastasis. In these advanced cases, chemotherapy and radiation have shown limited tumor control, and PC continues to be refractory to treatment and results in a poor survival outcome. In recent years, there has been intensive research on checkpoint inhibitor immunotherapy for PC, however, PC is characterized with dense stromal tissue and a tumor microenvironment (TME) that is highly immunosuppressive, which makes immunotherapy less effective. Interestingly, when immunotherapy is combined with radiation therapy (RT) and loco-regional hyperthermia (HT), it has demonstrated enhanced tumor responses. HT improves tumor killing via a variety of mechanisms, targeting both the tumor and the TME. Targeted HT raises the temperature of the tumor and surrounding tissues to 42⁻43 °C and makes the tumor more immunoresponsive. HT can also modulate the immune system of the TME by inducing and synthesizing heat shock proteins (HSP), which also activate an anti-tumor response. It is well known that HT can enhance RT-induced DNA damage in cancer cells and simultaneously help to oxygenate hypoxic regions. Thus, it is envisaged that combined HT and RT might have immunomodulatory effects in the PC-TME, making PC more responsive to immunotherapies. Moreover, the combined tripartite approach of immunotherapy, RT, and HT could reduce the overall toxicity associated with each individual therapy, while concomitantly enhancing the immunotherapeutic effect of overall individual therapies to treat local and metastatic PC. Thus, the use of a tripartite combinatorial approach could be promising and more efficacious than monotherapy or dual therapy to treat and increase the survival of the PC patients.
在所有癌症中,胰腺癌(PC)在男性和女性中的死亡率最高,所有阶段胰腺癌合并后的一年相对生存率为20%,五年相对生存率为8%。惠普尔手术,即胰十二指肠切除术,可提高可切除胰腺癌患者的生存率,然而,就诊时不到20%的患者适合手术。大多数患者被诊断为晚期胰腺癌,常伴有区域和远处转移。在这些晚期病例中,化疗和放疗对肿瘤的控制有限,胰腺癌仍然难以治疗,导致生存结果不佳。近年来,针对胰腺癌的检查点抑制剂免疫疗法进行了深入研究,然而,胰腺癌的特征是基质组织密集且肿瘤微环境(TME)具有高度免疫抑制性,这使得免疫疗法效果较差。有趣的是,当免疫疗法与放射治疗(RT)和局部区域热疗(HT)联合使用时,已显示出增强的肿瘤反应。热疗通过多种机制改善肿瘤杀伤,同时靶向肿瘤和肿瘤微环境。靶向热疗将肿瘤及周围组织的温度升高至42⁻43°C,使肿瘤更具免疫反应性。热疗还可通过诱导和合成热休克蛋白(HSP)来调节肿瘤微环境的免疫系统,这也会激活抗肿瘤反应。众所周知,热疗可增强放疗诱导的癌细胞DNA损伤,同时有助于为缺氧区域供氧。因此,可以设想,热疗和放疗联合可能在胰腺癌肿瘤微环境中具有免疫调节作用,使胰腺癌对免疫疗法更敏感。此外,免疫疗法、放疗和热疗的三联疗法可以降低与每种单一疗法相关的总体毒性,同时增强整体单一疗法治疗局部和转移性胰腺癌的免疫治疗效果。因此,使用三联组合疗法可能比单一疗法或双联疗法更有前景且更有效,可用于治疗并提高胰腺癌患者的生存率。