McCollum Rosalind, Taegtmeyer Miriam, Otiso Lilian, Muturi Nelly, Barasa Edwine, Molyneux Sassy, Martineau Tim, Theobald Sally
Department of International Public Health, Liverpool School of Tropical Medicine, Liverpool, UK.
LVCT Health, Nairobi, Kenya.
BMC Health Serv Res. 2018 Nov 29;18(1):906. doi: 10.1186/s12913-018-3706-5.
Practices of power lie at the heart of policy processes. In both devolution and priority-setting, actors seek to exert power through influence and control over material, human, intellectual and financial resources. Priority-setting arises as a consequence of the needs and demand exceeding the resources available, requiring some means of choosing between competing demands. This paper examines the use of power within priority-setting processes for healthcare resources at sub-national level, following devolution in Kenya.
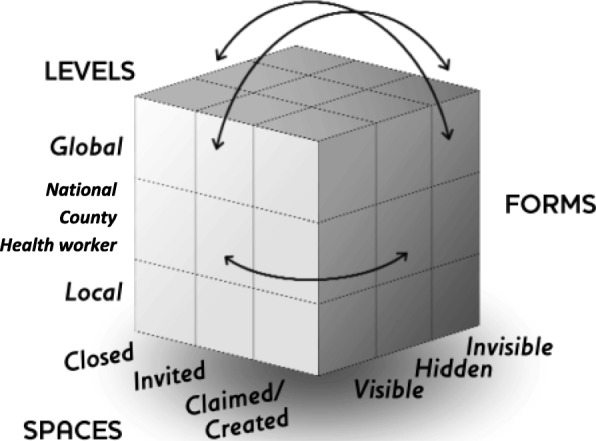
We interviewed 14 national level key informants and 255 purposively selected respondents from across the health system in ten counties. These qualitative data were supplemented by 14 focus group discussions (FGD) involving 146 community members in two counties. We conducted a power analysis using Gaventa's power cube and Veneklasen's expressions of power to interpret our findings.
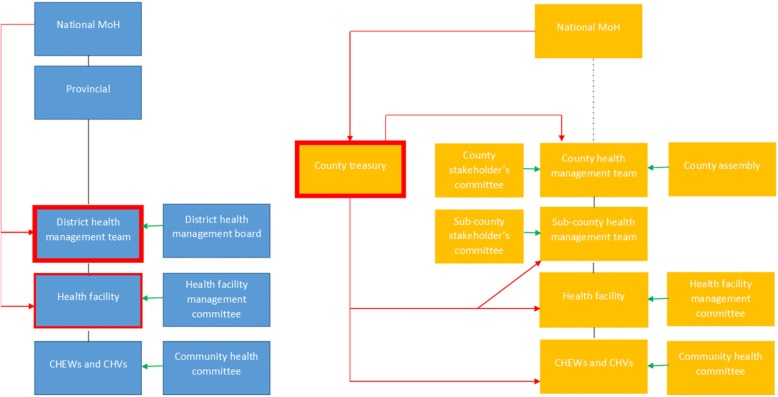
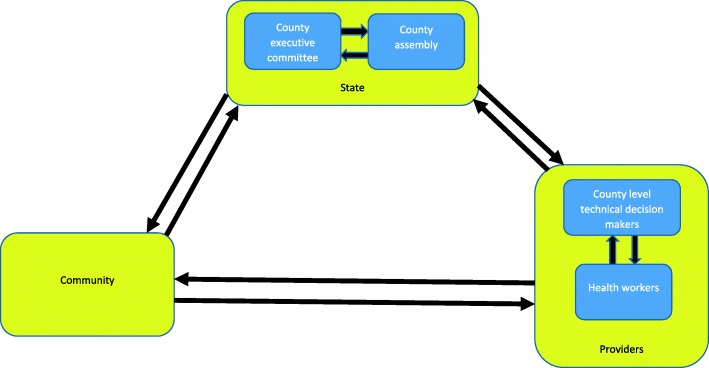
We found Kenya's transition towards devolution is transforming the former centralised balance of power, leading to greater ability for influence at the county level, reduced power at national and sub-county (district) levels, and limited change at community level. Within these changing power structures, politicians are felt to play a greater role in priority-setting for health. The interfaces and tensions between politicians, health service providers and the community has at times been felt to undermine health related technical priorities. Underlying social structures and discriminatory practices generally continue unchanged, leading to the continued exclusion of the most vulnerable from priority-setting processes.
Power analysis of priority-setting at county level after devolution in Kenya highlights the need for stronger institutional structures, processes and norms to reduce the power imbalances between decision-making actors and to enable community participation.
权力实践是政策过程的核心。在权力下放和确定优先事项的过程中,行为体试图通过对物质、人力、智力和财政资源的影响和控制来施加权力。由于需求超过了可用资源,需要某种方法在相互竞争的需求之间进行选择,因此确定优先事项应运而生。本文探讨了肯尼亚权力下放后,在国家以下层面的医疗资源优先事项确定过程中权力的运用情况。
我们采访了14名国家级关键信息提供者以及从十个县的卫生系统中特意挑选出的255名受访者。这些定性数据由涉及两个县146名社区成员的14次焦点小组讨论(FGD)加以补充。我们运用加文塔的权力立方体和韦内克拉森的权力表现形式进行了权力分析,以解读我们的研究结果。
我们发现,肯尼亚向权力下放的转变正在改变以前的中央集权权力平衡,导致县级影响力增强、国家和县级以下(区)权力减弱,而社区层面变化有限。在这些不断变化的权力结构中,人们认为政治家在卫生优先事项确定方面发挥着更大作用。政治家、卫生服务提供者和社区之间的接口与紧张关系有时被认为破坏了与卫生相关的技术优先事项。基本的社会结构和歧视性做法总体上仍未改变,导致最弱势群体在优先事项确定过程中继续被排除在外。
对肯尼亚权力下放后县级优先事项确定的权力分析凸显了建立更强大的体制结构、程序和规范的必要性,以减少决策行为体之间的权力不平衡,并促进社区参与。