McCollum Rosalind, Limato Ralalicia, Otiso Lilian, Theobald Sally, Taegtmeyer Miriam
Department of International Public Health, Liverpool School of Tropical Medicine, Liverpool, UK.
Eijkman Institute of Molecular Biology, Jakarta, Indonesia.
BMJ Glob Health. 2018 Sep 28;3(5):e000939. doi: 10.1136/bmjgh-2018-000939. eCollection 2018.
Devolution reforms in Indonesia and Kenya have brought extensive changes to governance structures and mechanisms for financing and delivering healthcare. Community health approaches can contribute towards attaining many of devolution's objectives, including community participation, responsiveness, accountability and improved equity. We set out to examine governance in two countries at different stages in the devolution journey: Indonesia at 15 years postdevolution and Kenya at 3 years.
We collected qualitative data across multiple levels of the health system in one district in Indonesia and ten counties in Kenya, through 80 interviews and six focus group discussions (FGD) in Indonesia and 269 interviews and 14 FGDs in Kenya. Qualitative data were digitally recorded, transcribed and coded before thematic framework analysis. Common themes between contexts were identified inductively and deductively, and similarities and differences critically analysed during an inter-country analysis workshop.
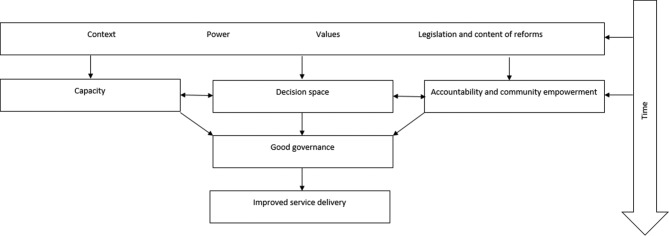
Following devolution both Indonesia and Kenya experienced similar challenges ensuring good governance for health. Devolution reforms transformed power relationships, increasing responsibilities at subnational levels and introducing opportunities for citizen participation. In both contexts, the impact of these mechanisms has been undermined by insufficiently clear guidance; failure to address pre-existing negative contextual norms and practices varied decision-maker values, limited priority-setting capacity and limited genuine community accountability. As a consequence, priorities in both contexts are too often placed on curative rather than preventive health services.
We recommend consideration of increased intersectoral actions that address social determinants of health, challenge negative norms and practices and place emphasis on community-based primary health services.
印度尼西亚和肯尼亚的权力下放改革给治理结构以及医疗保健融资与提供机制带来了广泛变革。社区卫生方法有助于实现权力下放的许多目标,包括社区参与、响应性、问责制和改善公平性。我们着手研究处于权力下放进程不同阶段的两个国家的治理情况:权力下放15年后的印度尼西亚和权力下放3年的肯尼亚。
我们通过在印度尼西亚一个地区进行80次访谈和6次焦点小组讨论(FGD),以及在肯尼亚10个县进行269次访谈和14次FGD,收集了印度尼西亚一个地区和肯尼亚10个县卫生系统多个层面的定性数据。定性数据在进行主题框架分析之前进行了数字记录、转录和编码。通过归纳和演绎确定了不同背景之间的共同主题,并在一次国家间分析研讨会上对异同点进行了批判性分析。
权力下放后,印度尼西亚和肯尼亚在确保卫生领域良好治理方面都面临类似挑战。权力下放改革改变了权力关系,增加了地方各级的责任,并为公民参与创造了机会。在这两种情况下,这些机制的影响都因指导不够明确、未能解决先前存在的负面背景规范和做法、决策者价值观各异、优先事项设定能力有限以及真正的社区问责制有限而受到削弱。因此,在这两种情况下,往往将重点放在治疗性而非预防性卫生服务上。
我们建议考虑加强跨部门行动,以解决健康的社会决定因素、挑战负面规范和做法,并强调以社区为基础的初级卫生服务。