Santoro Lore, Mora-Ramirez Erick, Trauchessec Dorian, Chouaf Soufiane, Eustache Pierre, Pouget Jean-Pierre, Kotzki Pierre-Olivier, Bardiès Manuel, Deshayes Emmanuel
Nuclear Medicine Department, Montpellier Cancer Institute (ICM), University of Montpellier, 208 Avenue des Apothicaires, 34298, Montpellier Cedex5, France.
Centre de Recherche en Cancérologie de Toulouse, Toulouse, France.
EJNMMI Res. 2018 Nov 29;8(1):103. doi: 10.1186/s13550-018-0459-4.
This study's aim was to develop our dosimetric methodology using a commercial workstation for the routine evaluation of the organs at risk during peptide receptor radionuclide therapy (PRRT) with Lu.
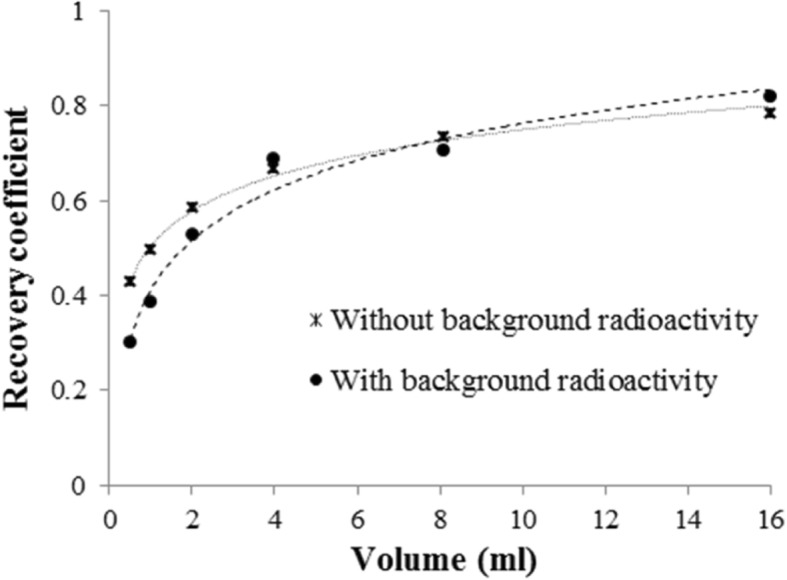
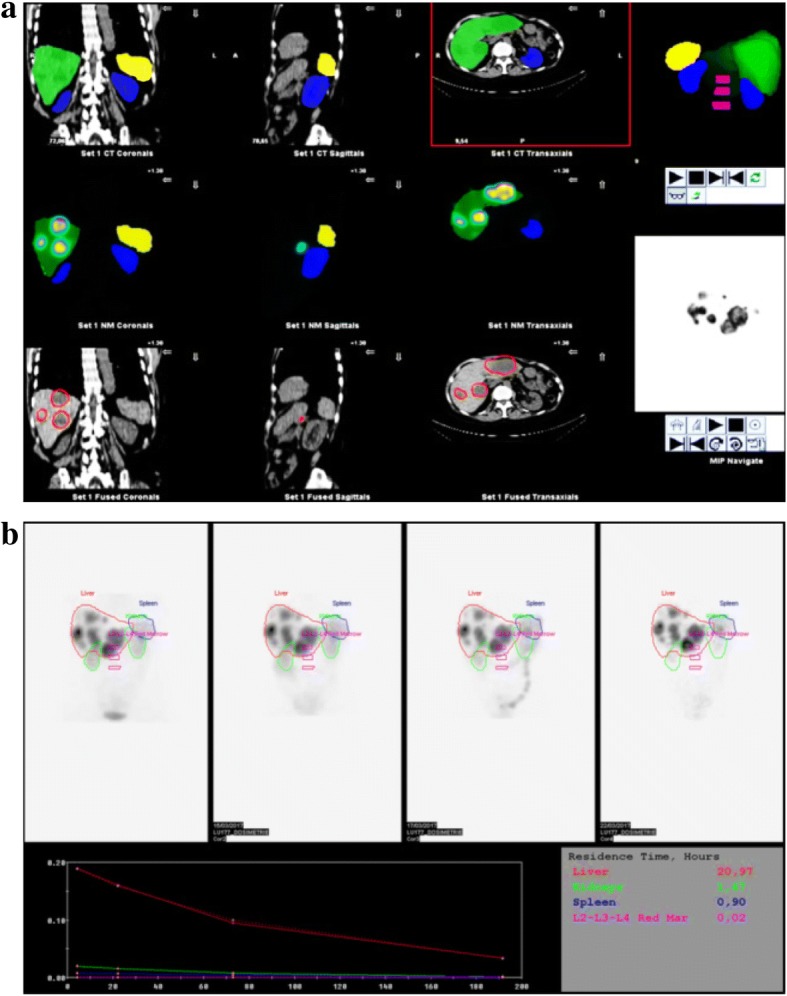
First, planar and SPECT sensitivity factors were determined on phantoms. The reconstruction parameters were optimized by SPECT/CT image acquisition using a NEMA IEC phantom containing a 500 ml bottle of Lu, to simulate a kidney. The recovery coefficients were determined on various phantoms. For the red marrow, this was calculated using a NEMA IEC phantom that contained a centrally placed bottle of 80 ml of Lu (to model the L2-L4 red marrow) flanked by two 200 ml bottles with Lu to simulate the kidneys. Then, SPECT/CT images were acquired at 4, 24, 72, and 192 h after injection in 12 patients with neuroendocrine tumors who underwent PRRT with Lu-DOTATATE. SPECT data were reconstructed using the iterative ordered subset expectation maximization (OSEM) method, with six iterations and ten subsets, attenuation, scatter, recovery resolution corrections, and a Gaussian post-filter of 0.11 cm. The liver, spleen, kidneys, and red marrow dose per administered activity (AD/A admin) values were calculated with the Medical Internal Radiation Dose (MIRD) formalism and the residence times (Dosimetry toolkit® application) using standard and CT imaging-based organ masses (OLINDA/EXM® V1.0 software).
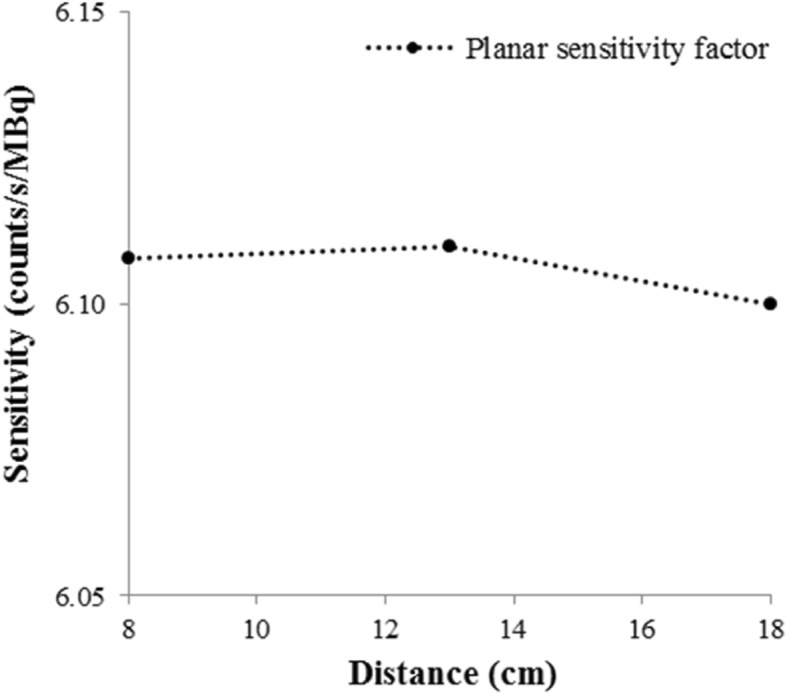
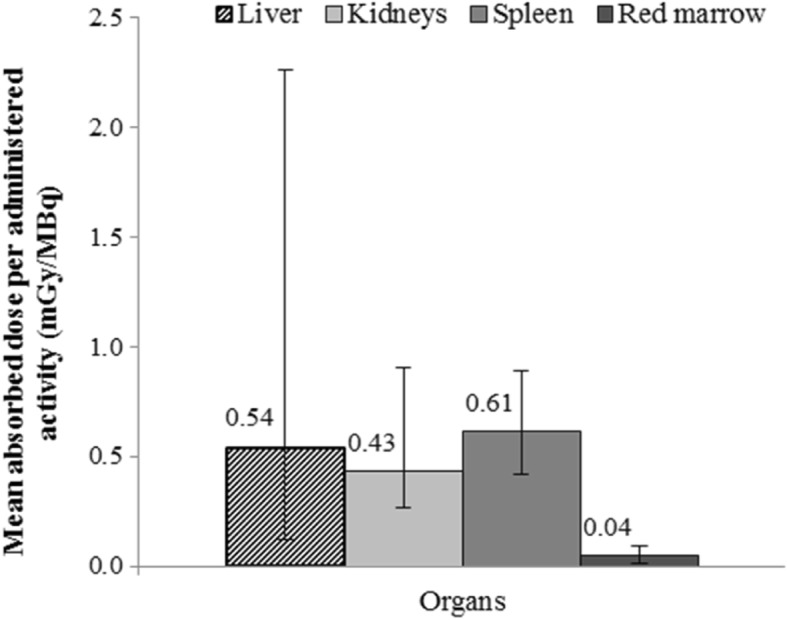
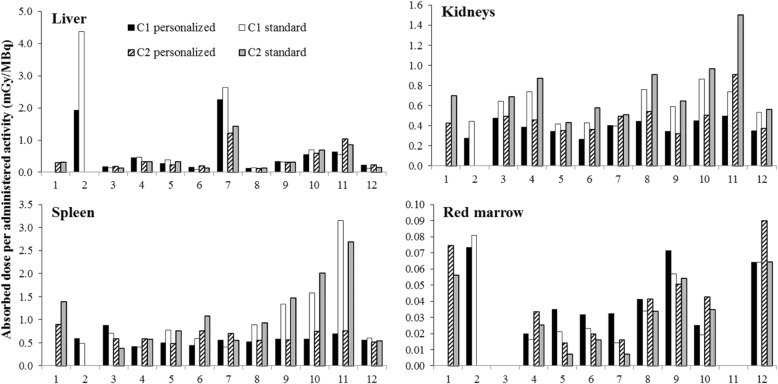
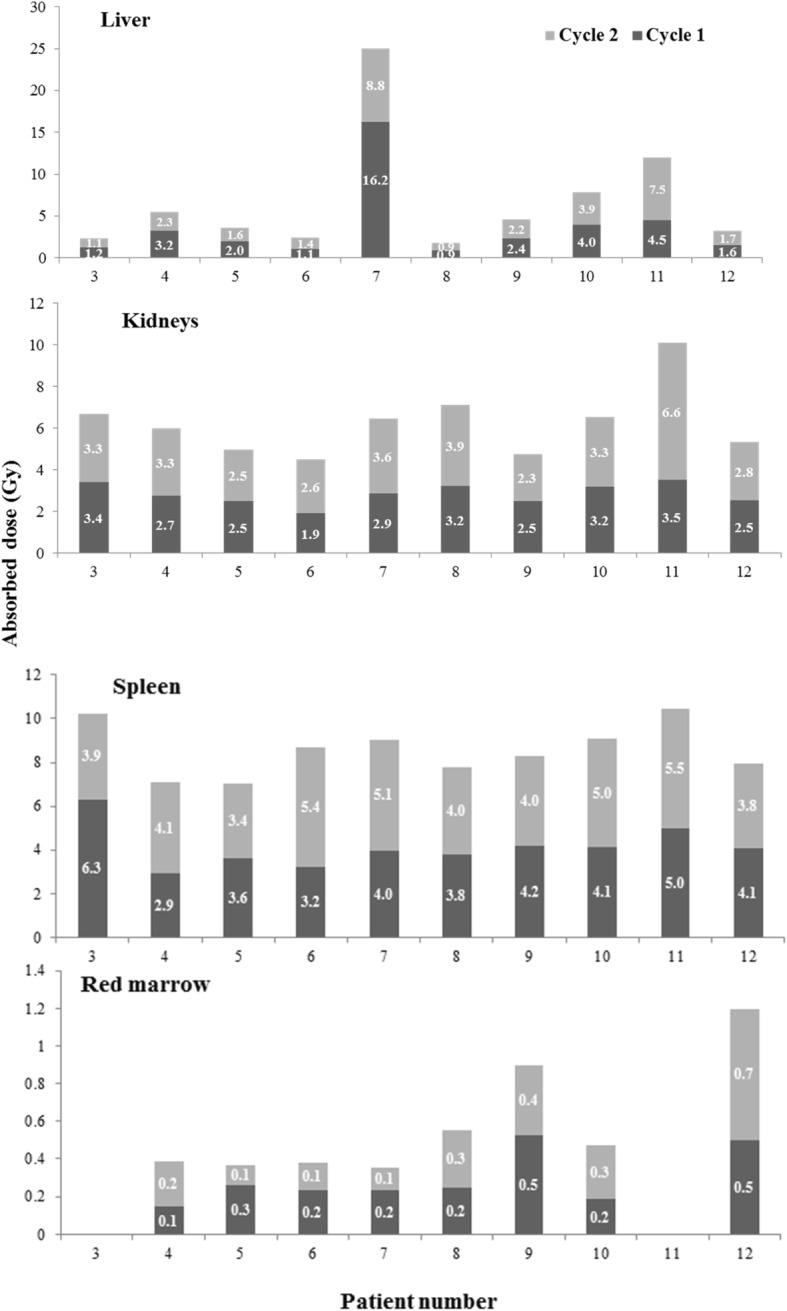
Sensitivity factors of 6.11 ± 0.01 and 5.67 ± 0.08 counts/s/MBq were obtained with planar and SPECT/CT acquisitions, respectively. A recovery coefficient of 0.78 was obtained for the modeled L2-L4 red marrow. The mean AD/A admin values were 0.43 ± 0.13 mGy/MBq [0.27-0.91] for kidneys, 0.54 ± 0.58 mGy/MBq [0.12-2.26] for liver, 0.61 ± 0.13 mGy/MBq [0.42-0.89] for spleen, and 0.04 ± 0.02 mGy/MBq [0.01-0.09] for red marrow. The AD/A admin values varied when calculated using the personalized and standard organ mass, particularly for kidneys (p = 1 × 10), spleen (p = 0.0069), and red marrow (p = 0.0027). Intra-patient differences were observed especially in organs close to or including tumor cells or metastases.
The obtained AD/A admin values were in agreement with the literature data. This study shows the technical feasibility of patient dosimetry in clinical practice and the need to obtain patient-specific information.
本研究的目的是开发一种使用商用工作站的剂量测定方法,用于在使用镥进行肽受体放射性核素治疗(PRRT)期间对危及器官进行常规评估。
首先,在体模上确定平面和SPECT灵敏度因子。通过使用包含一瓶500毫升镥的NEMA IEC体模进行SPECT/CT图像采集来优化重建参数,以模拟肾脏。在各种体模上确定恢复系数。对于红骨髓,使用NEMA IEC体模计算,该体模包含一瓶位于中心的80毫升镥(模拟L2-L4红骨髓),两侧各有两瓶200毫升的镥以模拟肾脏。然后,在12例接受镥- DOTATATE PRRT的神经内分泌肿瘤患者注射后4、24、72和192小时采集SPECT/CT图像。使用迭代有序子集期望最大化(OSEM)方法重建SPECT数据,进行六次迭代和十个子集,进行衰减、散射、恢复分辨率校正,并使用0.11厘米的高斯后置滤波器。使用医学内部辐射剂量(MIRD)形式和驻留时间(剂量测定工具包®应用程序),使用基于标准和CT成像的器官质量(OLINDA/EXM® V1.0软件)计算肝脏、脾脏、肾脏和每给药活度(AD/A给药)的红骨髓剂量值。
平面和SPECT/CT采集分别获得的灵敏度因子为6.11±0.01和5.67±0.08计数/秒/MBq。模拟的L2-L4红骨髓的恢复系数为0.78。肾脏的平均AD/A给药值为0.43±0.13 mGy/MBq [0.27 - 0.91],肝脏为0.54±0.58 mGy/MBq [0.12 - 2.26],脾脏为0.61±0.13 mGy/MBq [0.42 - 0.89],红骨髓为0.04±0.02 mGy/MBq [0.01 - 0.09]。使用个性化和标准器官质量计算时,AD/A给药值有所不同,特别是对于肾脏(p = 1×10)、脾脏(p = 0.0069)和红骨髓(p = 0.0027)。在患者体内观察到差异,特别是在靠近或包括肿瘤细胞或转移灶的器官中。
获得的AD/A给药值与文献数据一致。本研究表明了患者剂量测定在临床实践中的技术可行性以及获取患者特异性信息的必要性。