Verbeek Thomas A, Stine Jonathan G, Saner Fuat H, Bezinover Dmitri
Department of Anesthesiology and Perioperative Medicine, The Pennsylvania State University-Milton S. Hershey Medical Center, Hershey, PA.
Division of Gastroenterology & Hepatology, Department of Medicine, The Pennsylvania State University-Milton S. Hershey Medical Center, Hershey, PA.
Transplant Direct. 2018 Oct 26;4(11):e403. doi: 10.1097/TXD.0000000000000843. eCollection 2018 Nov.
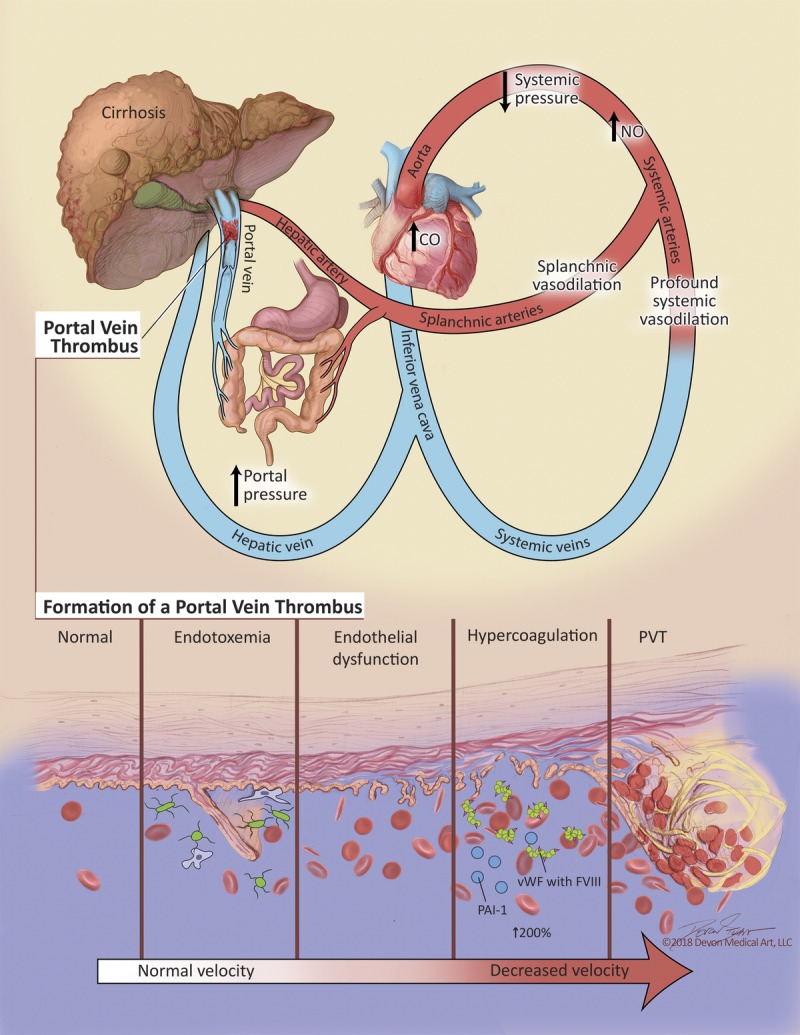
In this review, we analyze the epidemiology of thromboses related to end-stage liver disease (ESLD), discuss causes of hypercoagulability, describe susceptible populations, and critically evaluate proposed prophylaxis and treatment of thromboses. Classically, ESLD has been regarded as a model for coagulopathy, and patients were deemed to be at high risk for bleeding complications. Patients with ESLD are not auto-anticoagulated, and they do not have a lower risk of portal vein thrombosis, intracardiac thrombus formation, pulmonary embolism or hepatic artery thrombosis. Though the cause of hypercoagulability is multifactorial, endothelial dysfunction likely plays a central role for all patients with ESLD. Some subpopulations, such as patients with nonalcoholic steatohepatitis and autoimmune conditions, are at increased risk of thrombotic events as are patients of Hispanic ethnicity. The science behind prophylaxis of different types of clotting and treatment of thromboses is developing rapidly. A number of medications, including low molecular weight heparin, unfractionated heparin, aspirin, vitamin K antagonists, and direct oral anticoagulants can be used, but clear guidelines are lacking. Acute intraoperative clotting can be associated with high mortality. Routine use of transesophageal echocardiography can be helpful in early recognition and treatment of intraoperative thrombosis. Heparin should be reserved for cases of intracardiac thrombus/pulmonary embolism without hemodynamic instability. In unstable patients, low dose of recombinant tissue plasminogen activator can be used. In this new era of heightened awareness of thrombotic events in ESLD patients, prospective randomized trials are urgently needed to best guide clinical practice.
在本综述中,我们分析了终末期肝病(ESLD)相关血栓形成的流行病学,讨论了高凝状态的原因,描述了易感人群,并严格评估了针对血栓形成的预防性治疗和治疗方案。传统上,ESLD被视为凝血病的一个模型,患者被认为有发生出血并发症的高风险。ESLD患者并非自身抗凝,他们发生门静脉血栓形成、心内血栓形成、肺栓塞或肝动脉血栓形成的风险并不低。尽管高凝状态的原因是多因素的,但内皮功能障碍可能在所有ESLD患者中起核心作用。一些亚组人群,如非酒精性脂肪性肝炎患者和自身免疫性疾病患者,以及西班牙裔患者发生血栓事件的风险增加。针对不同类型凝血的预防措施及血栓治疗的相关科学正在迅速发展。包括低分子量肝素、普通肝素、阿司匹林、维生素K拮抗剂和直接口服抗凝剂在内的多种药物均可使用,但缺乏明确的指南。术中急性凝血可能与高死亡率相关。常规使用经食管超声心动图有助于术中血栓形成的早期识别和治疗。肝素应保留用于无血流动力学不稳定的心内血栓/肺栓塞病例。对于不稳定患者,可使用低剂量重组组织型纤溶酶原激活剂。在这个对ESLD患者血栓事件关注度提高的新时代,迫切需要前瞻性随机试验来更好地指导临床实践。