Graves Kevin G, May Heidi T, Knowlton Kirk U, Muhlestein Joseph B, Jacobs Victoria, Lappé Donald L, Anderson Jeffrey L, Horne Benjamin D, Bunch Thomas Jared
Intermountain Heart Institute, Intermountain Medical Center, Murray, Utah, USA.
Cardiology Division, Department of Internal Medicine, University of Utah, Murray, Utah, USA.
Open Heart. 2018 Nov 17;5(2):e000907. doi: 10.1136/openhrt-2018-000907. eCollection 2018.
Oral anticoagulation (OAC) therapy guidelines recommend using CHADS-VASc to determine OAC need in atrial fibrillation (AF). A usable tool, CHADS-VASc is challenged by its predictive ability. Applying components of the complete blood count and basic metabolic profile, the Intermountain Mortality Risk Score (IMRS) has been extensively validated. This study evaluated whether use of IMRS with CHADS-VASc in patients with AF improves prediction.
Patients with AF undergoing cardiac catheterisation (N=10 077) were followed for non-fatal stroke and mortality (mean 5.8±4.1 years, maximum 19 years). CHADS-VASc and IMRS were calculated at baseline. IMRS categories were defined based on previously defined criteria. Cox regression was adjusted for demographic, clinical and treatment variables not included in IMRS or CHADS-VASc.
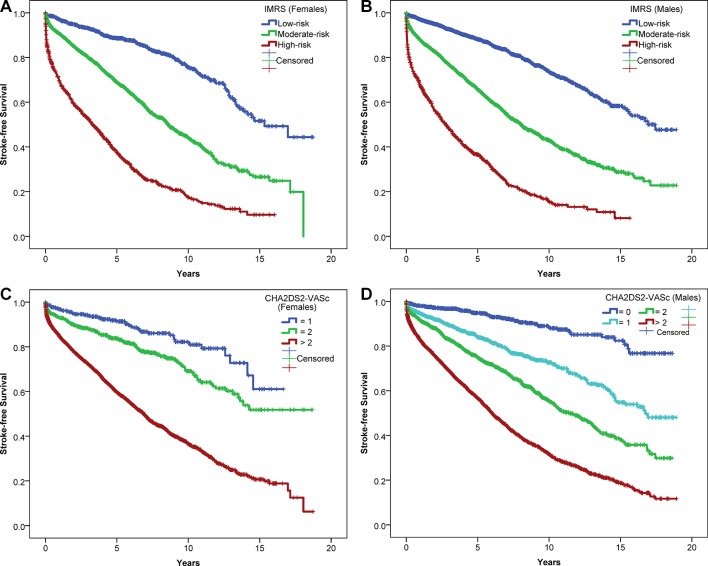
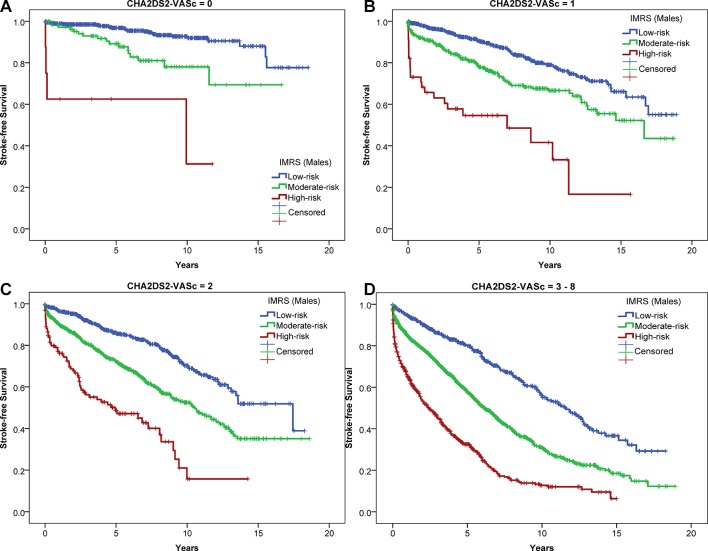
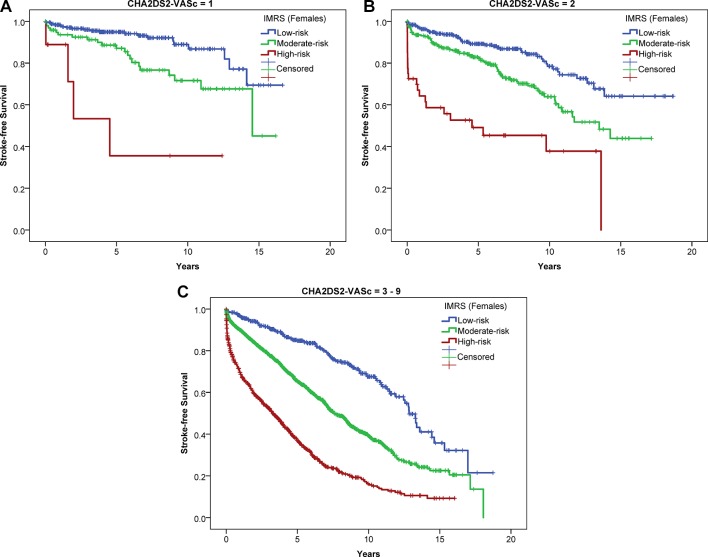
In women (n=4122, mean age 71±12 years), the composite of non-fatal stroke/mortality was stratified (all p-trend <0.001) by CHADS-VASc (1: 12.6%, 2: 22.8%, >2: 48.1%) and IMRS (low: 17.8%, moderate: 40.9%, high risk: 64.5%), as it was for men (n=5955, mean age 68±12 years) by CHADS-VASc (<2: 15.7%, 2: 30.3%, >2: 51.8%) and IMRS (low: 19.0%, moderate: 42.0%, high risk: 65.9%). IMRS stratified stroke/mortality (all p-trend <0.001) in each CHADS-VASc category.
Using IMRS jointly with CHADS-VASc in patients with AF improved the prediction of stroke and mortality. For example, in patients at the OAC treatment threshold (CHADS -VASc = 2), IMRS provided ≈4-fold separation between low and high risk. IMRS provides an enhancing marker for risk in patients with AF that reflects the underlying systemic nature of this disease that may be considered in combination with the CHADS-VASc score.
口服抗凝(OAC)治疗指南推荐使用CHADS-VASc评分来确定房颤(AF)患者是否需要进行OAC治疗。作为一种可用的工具,CHADS-VASc评分的预测能力受到质疑。利用全血细胞计数和基本代谢指标的组成部分,山间死亡率风险评分(IMRS)已得到广泛验证。本研究评估了在房颤患者中联合使用IMRS和CHADS-VASc评分是否能改善预测效果。
对接受心导管检查的房颤患者(N = 10077例)进行随访,观察非致死性卒中及死亡率(平均5.8±4.1年,最长19年)。在基线时计算CHADS-VASc评分和IMRS评分。IMRS类别根据先前定义的标准确定。Cox回归针对IMRS或CHADS-VASc评分未纳入的人口统计学、临床和治疗变量进行了校正。
在女性患者(n = 4122例,平均年龄71±12岁)中,非致死性卒中/死亡率的复合终点根据CHADS-VASc评分分层(所有p趋势<0.001)(1分:12.6%,2分:22.8%,>2分:48.1%),根据IMRS评分分层(低风险:17.8%,中度风险:40.9%,高风险:64.5%);男性患者(n = 5955例,平均年龄68±12岁)同样如此,根据CHADS-VASc评分分层(<2分:15.7%,2分:30.3%,>2分:51.8%),根据IMRS评分分层(低风险:19.0%,中度风险:42.0%,高风险:65.9%)。在每个CHADS-VASc评分类别中,IMRS均能对卒中/死亡率进行分层(所有p趋势<0.001)。
在房颤患者中联合使用IMRS和CHADS-VASc评分可改善对卒中和死亡率的预测。例如,在OAC治疗阈值(CHADS-VASc = 2)的患者中,IMRS在低风险和高风险之间提供了约4倍的区分度。IMRS为房颤患者的风险提供了一个增强指标,反映了该疾病潜在的全身性本质,可与CHADS-VASc评分联合考虑。