Ouologuem Dinkorma T, Kone Cheick O, Fofana Bakary, Sidibe Bakary, Togo Amadou H, Dembele Demba, Toure Sekou, Koumare Sekou, Toure Ousmane, Sagara Issaka, Toure Abdoulaye, Dao Adama, Doumbo Ogobara K, Djimde Abdoulaye A
Malaria Research and Training Center, Department of Epidemiology of Parasitic Diseases, University of Science, Techniques and Technologies of Bamako, Bamako, Mali.
Afr J Lab Med. 2018 Dec 6;7(2):784. doi: 10.4102/ajlm.v7i2.784. eCollection 2018.
Most malaria-endemic countries use artemisinin-based combination therapy (ACT) as their first-line treatment. ACTs are known to be highly effective on asexual stages of the malaria parasite. Malaria transmission and the spread of resistant parasites depend on the infectivity of gametocytes. The effect of the current ACT regimens on gametocyte infectivity is unclear.
This study aimed to determine the infectivity of gametocytes to following ACT treatment in the field.
During a randomised controlled trial in Bougoula-Hameau, Mali, conducted from July 2005 to July 2007, volunteers with uncomplicated malaria were randomised to receive artemether-lumefantrine, artesunate-amodiaquine, or artesunate-sulfadoxine/pyrimethamine. Volunteers were followed for 28 days, and gametocyte carriage was assessed. Direct skin feeding assays were performed on gametocyte carriers before and after ACT administration.
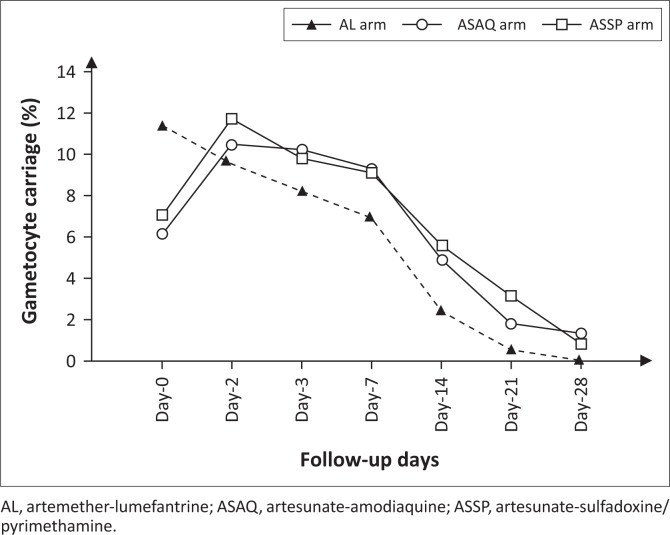
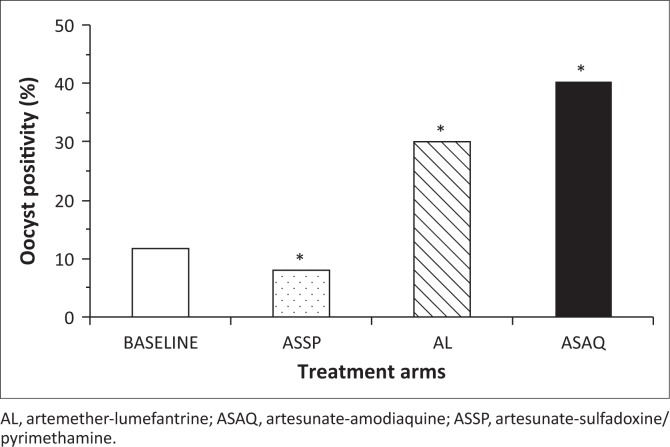
Following artemether-lumefantrine treatment, gametocyte carriage decreased steadily from Day 0 to Day 21 post-treatment initiation. In contrast, for the artesunate-amodiaquine and artesunate-sulfadoxine/pyrimethamine arms, gametocyte carriage increased on Day 3 and remained constant until Day 7 before decreasing afterward. Mosquito feeding assays showed that artemether-lumefantrine and artesunate-amodiaquine significantly increased gametocyte infectivity to (s.l.) ( < 10), whereas artesunate-sulfadoxine/pyrimethamine decreased gametocyte infectivity in this setting ( = 0.03).
Different ACT regimens could lead to gametocyte populations with different capacity to infect the vector. Frequent assessment of the effect of antimalarials on gametocytogenesis and gametocyte infectivity may be required for the full assessment of treatment efficacy, the potential for spread of drug resistance and malaria transmission in the field.
大多数疟疾流行国家将以青蒿素为基础的联合疗法(ACT)作为一线治疗方法。已知ACT对疟原虫的无性阶段非常有效。疟疾传播和耐药寄生虫的传播取决于配子体的传染性。目前的ACT方案对配子体传染性的影响尚不清楚。
本研究旨在确定在实地接受ACT治疗后配子体的传染性。
在2005年7月至2007年7月于马里布古拉-哈莫进行的一项随机对照试验中,将患有非复杂性疟疾的志愿者随机分为接受蒿甲醚-本芴醇、青蒿琥酯-阿莫地喹或青蒿琥酯-磺胺多辛/乙胺嘧啶治疗。对志愿者进行28天的随访,并评估配子体携带情况。在给予ACT前后,对配子体携带者进行直接皮肤接种试验。
接受蒿甲醚-本芴醇治疗后,配子体携带率从治疗开始后的第0天到第21天稳步下降。相比之下,对于青蒿琥酯-阿莫地喹组和青蒿琥酯-磺胺多辛/乙胺嘧啶组,配子体携带率在第3天增加,并在第7天之前保持不变,之后下降。蚊虫接种试验表明,蒿甲醚-本芴醇和青蒿琥酯-阿莫地喹显著增加了配子体对(按蚊属)(狭义)的传染性(P<0.01),而在这种情况下青蒿琥酯-磺胺多辛/乙胺嘧啶降低了配子体的传染性(P=0.03)。
不同的ACT方案可能导致配子体群体对传播媒介的感染能力不同。为了全面评估治疗效果、耐药性传播的可能性以及实地疟疾传播情况,可能需要经常评估抗疟药对配子体发生和配子体传染性的影响。