From the Saint Vincent Hospital, Department of Internal Medicine, Worcester, MA (Z.H.).
University of Pennsylvania Perelman School of Medicine, Center for Magnetic Resonance and Optical Imaging, Philadelphia (J.L., S.G., G.O., I.V., J.A.C.).
Hypertension. 2019 Feb;73(2):364-370. doi: 10.1161/HYPERTENSIONAHA.118.12157.
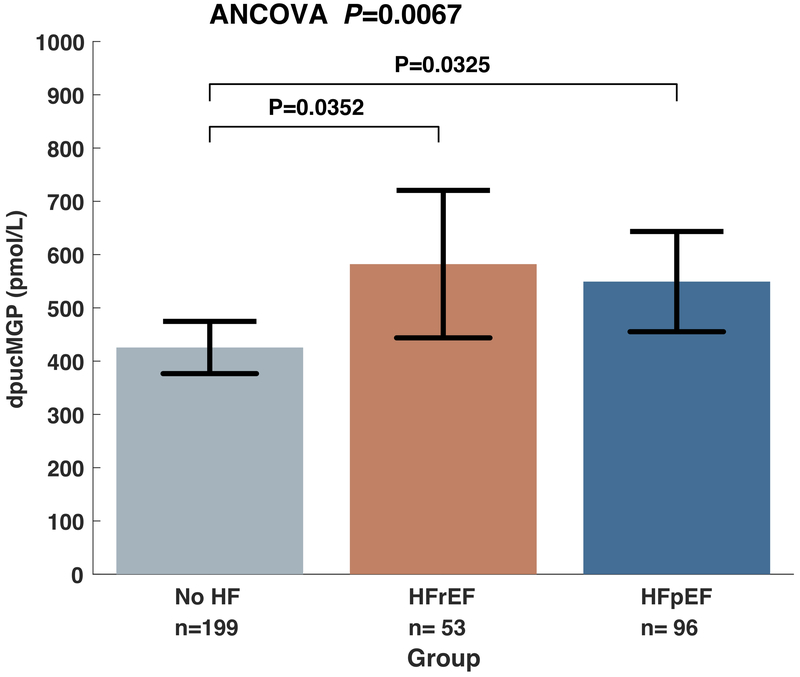
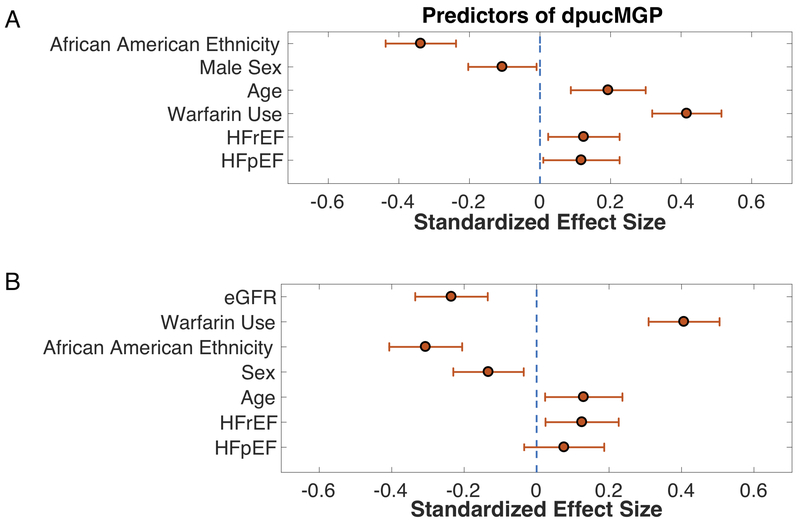
Large artery stiffening contributes to the pathophysiology of heart failure (HF) and associated comorbidities. MGP (matrix Gla-protein) is a potent inhibitor of vascular calcification. MGP activation is vitamin K-dependent. We aimed (1) to compare dp-ucMGP (dephospho-uncarboxylated MGP) levels between subjects with HF with preserved ejection fraction (HFpEF) and HF with reduced ejection fraction (HFrEF) and subjects without HF; (2) to assess the relationship between dp-ucMGP levels and arterial stiffness; and (3) to assess the relationship between warfarin use, dp-ucMGP levels, and arterial stiffness in HF. We enrolled 348 subjects with HFpEF (n=96), HFrEF (n=53), or no HF (n=199). Carotid-femoral pulse wave velocity, a measure of large artery stiffness, was measured with arterial tonometry. Dp-ucMGP was measured with ELISA. Dp-ucMGP levels were greater in both HFrEF (582 pmol/L; 95% CI, 444-721 pmol/L) and HFpEF (549 pmol/L; 95% CI, 455-643 pmol/L) compared with controls (426 pmol/L; 95% CI, 377-475 pmol/L; ANCOVA P=0.0067). Levels of dp-ucMGP were positively associated with carotid-femoral pulse wave velocity (standardized β, 0.31; 95% CI, 0.19-0.42; P<0.0001), which was also true in analyses restricted to patients with HF (standardized β, 0.34; 95% CI, 0.16-0.52; P=0.0002). Warfarin use was significantly associated with carotid-femoral pulse wave velocity (standardized β, 0.13; 95% CI, 0.004-0.26; P=0.043), but this relationship was eliminated after adjustment for dp-ucMGP. In conclusion, levels of dp-ucMGP are increased in HFpEF and HFrEF and are independently associated with arterial stiffness. Future studies should investigate whether vitamin K supplementation represents a suitable therapeutic strategy to prevent or reduce arterial stiffness in HFpEF and HFrEF.
大动脉僵硬是心力衰竭(HF)及其相关合并症的病理生理学基础。MGP(基质 Gla 蛋白)是一种有效的血管钙化抑制剂。MGP 的激活依赖于维生素 K。我们的目的是:(1)比较射血分数保留型心力衰竭(HFpEF)、射血分数降低型心力衰竭(HFrEF)与无心力衰竭患者之间 dp-ucMGP(脱磷酸非羧化 MGP)水平的差异;(2)评估 dp-ucMGP 水平与动脉僵硬之间的关系;(3)评估华法林使用、dp-ucMGP 水平与心力衰竭患者动脉僵硬之间的关系。我们共纳入了 348 名 HFpEF(n=96)、HFrEF(n=53)或无心力衰竭(n=199)患者。使用动脉张力测定法测量颈动脉-股动脉脉搏波速度,以评估大动脉僵硬程度。通过 ELISA 法测量 dp-ucMGP 水平。与对照组相比,HFrEF(582pmol/L;95%CI,444-721pmol/L)和 HFpEF(549pmol/L;95%CI,455-643pmol/L)患者的 dp-ucMGP 水平均显著升高(ANCOVA,P=0.0067)。dp-ucMGP 水平与颈动脉-股动脉脉搏波速度呈正相关(标准化β=0.31;95%CI,0.19-0.42;P<0.0001),该相关性在仅纳入心力衰竭患者的分析中同样成立(标准化β=0.34;95%CI,0.16-0.52;P=0.0002)。华法林的使用与颈动脉-股动脉脉搏波速度显著相关(标准化β=0.13;95%CI,0.004-0.26;P=0.043),但在调整 dp-ucMGP 水平后,这种相关性消失了。总之,HFpEF 和 HFrEF 患者的 dp-ucMGP 水平升高,且与动脉僵硬独立相关。未来的研究应探讨维生素 K 补充是否代表一种合适的治疗策略,以预防或降低 HFpEF 和 HFrEF 患者的动脉僵硬程度。