Wei Ke, Min Su, Hao Yonggang, Ran Wei, Lv Feng
Department of Anesthesiology, The First Affiliated Hospital of Chongqing Medical University, Chongqing, People's Republic of China,
J Pain Res. 2018 Dec 18;12:29-37. doi: 10.2147/JPR.S188568. eCollection 2019.
Judicious postoperative pain management after thoracoscopic-laparoscopic esophagectomy (TLE) facilitates enhanced rehabilitation. Thoracic epidural analgesia (TEA) offers many benefits in esophagectomy, while several complications are associated with the delivery mode by continuous epidural infusion. This study compared the efficiency and safety of intermittent epidural bolus to continuous epidural infusion for pain management after TLE.
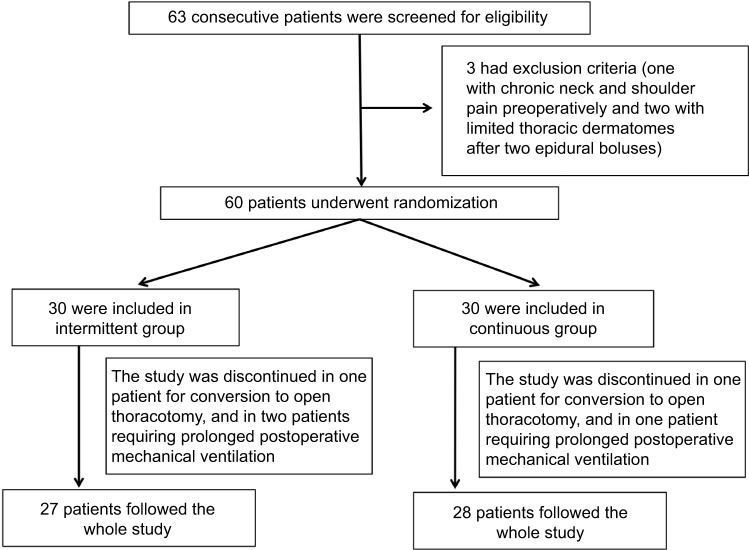
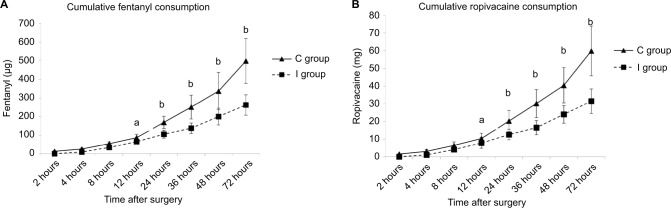
Sixty patients, aged 18-80 years, with American Society of Anesthesiologists classes I-III and scheduled for TLE with combined general anesthesia and TEA were randomly allocated to two groups. Patients received either a continuous epidural infusion with 0.3% ropivacaine and 1.5 µg/mL fentanyl at 6 mL/h plus a patient-controlled bolus of 3 mL (continuous group) or an intermittent bolus of 6 mL of the same solution on demand with lockout time of 30 minutes (intermittent group). If the patient complained of pain and the visual analog scale score was >4, an intravenous injection of tramadol or dezocine was administered as rescue treatment. The primary outcome variable was the consumption of epidural opioids and local anesthetics for TEA.
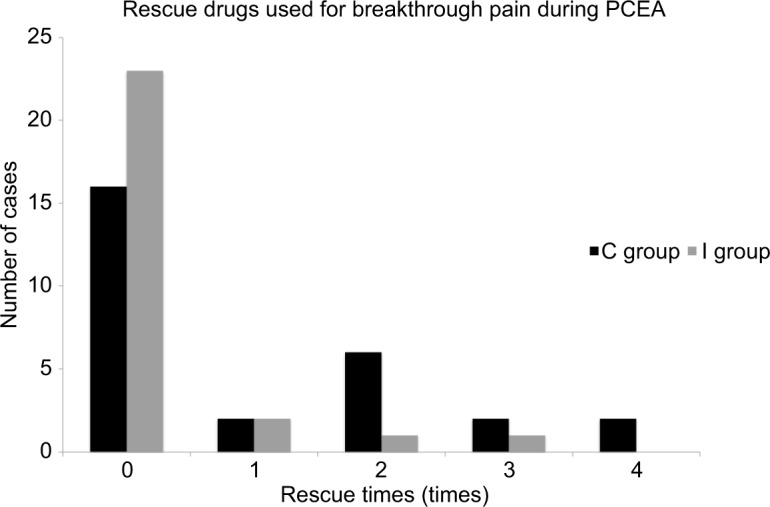
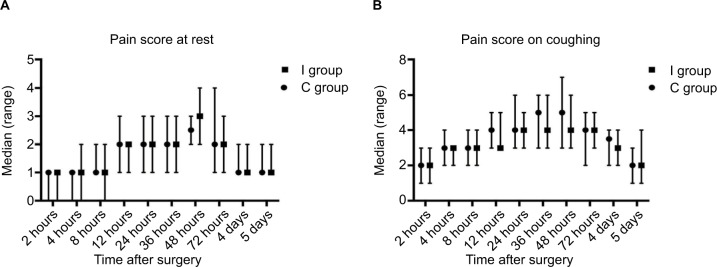
TEA for pain management following TLE by intermittent epidural bolus was associated with significantly lower consumption of fentanyl and ropivacaine and lower incidences of breakthrough pain and hypotension than continuous epidural infusion. No significant differences were observed between the two groups in terms of pain score at rest or while coughing, patient satisfaction, or incidence of postoperative complications.
Compared with continuous epidural infusion, TEA by on-demand intermittent bolus greatly reduced the consumption of local anesthetics and opioids with comparable pain relief and little impairment in hemodynamics when used for pain management after TLE.
胸腔镜-腹腔镜联合食管癌切除术(TLE)术后合理的疼痛管理有助于促进康复。胸段硬膜外镇痛(TEA)在食管癌切除术中具有诸多益处,然而连续硬膜外输注的给药方式会引发一些并发症。本研究比较了间歇性硬膜外推注与连续硬膜外输注用于TLE术后疼痛管理的有效性和安全性。
60例年龄在18 - 80岁、美国麻醉医师协会分级为I - III级、计划接受全身麻醉联合TEA的TLE患者被随机分为两组。患者分别接受以6 mL/h的速度持续硬膜外输注0.3%罗哌卡因和1.5 μg/mL芬太尼并加用3 mL患者自控推注(连续组),或按需间歇性推注6 mL相同溶液且锁定时间为30分钟(间歇组)。如果患者主诉疼痛且视觉模拟评分>4,则静脉注射曲马多或地佐辛作为补救治疗。主要观察变量是TEA时硬膜外阿片类药物和局部麻醉药的消耗量。
与连续硬膜外输注相比,间歇性硬膜外推注用于TLE术后疼痛管理时,芬太尼和罗哌卡因的消耗量显著更低,爆发痛和低血压的发生率也更低。两组在静息或咳嗽时的疼痛评分、患者满意度或术后并发症发生率方面未观察到显著差异。
与连续硬膜外输注相比,按需间歇性推注的TEA用于TLE术后疼痛管理时,能显著减少局部麻醉药和阿片类药物的消耗量,在疼痛缓解效果相当的情况下,对血流动力学的影响较小。