Borean Michael, Shani Kishan, Brown M Catherine, Chen Judy, Liang Mindy, Karkada Joel, Kooner Simranjit, Doherty Mark K, O'Kane Grainne M, Jang Raymond, Elimova Elena, Wong Rebecca K, Darling Gail E, Xu Wei, Howell Doris, Liu Geoffrey
Division of Medical Oncology Princess Margaret Cancer Centre and Departments of Medicine and Epidemiology, Dalla Lana School of Public Health University of Toronto Toronto Ontario Canada.
Odette Cancer Centre University of Toronto Toronto Ontario Canada.
Health Sci Rep. 2018 May 21;1(7):e48. doi: 10.1002/hsr2.48. eCollection 2018 Jul.
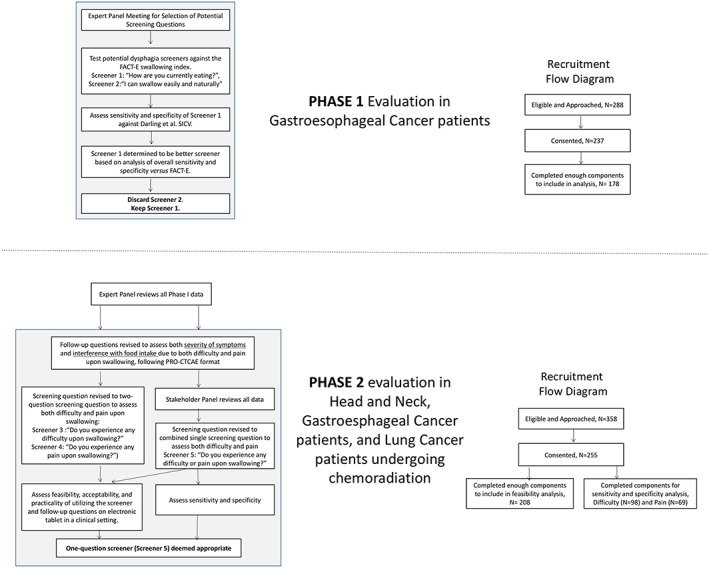
Dysphagia can be associated with significant morbidity in cancer patients. We aimed to develop and evaluate dysphagia screener tools for use in observational studies (phase 1) and for routine symptom monitoring in clinical care (phase 2).
Various dysphagia or odynophagia screening questions, selected after an expert panel reviewed the content, criterion, and construct validity, were compared with either functional assessment of cancer therapy - esophageal cancer (FACT-E) Swallowing Index Cut-Off Values or to questions adapted from the Patient Reported Outcomes for Common Terminology Criteria for Adverse Events. Sensitivity, specificity, and patient acceptability were assessed.
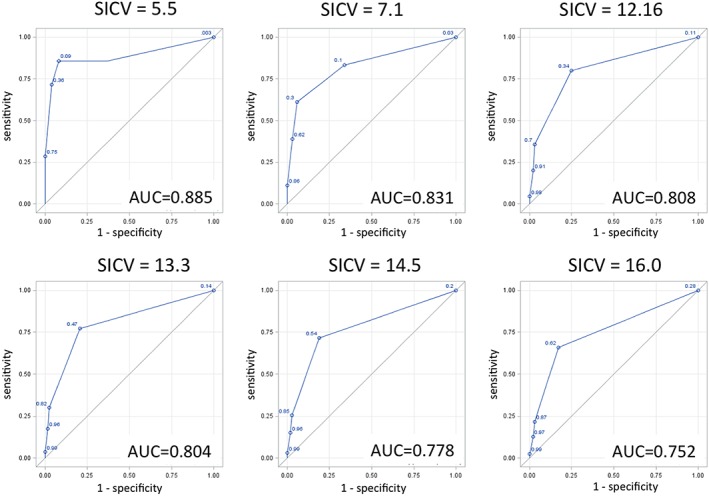
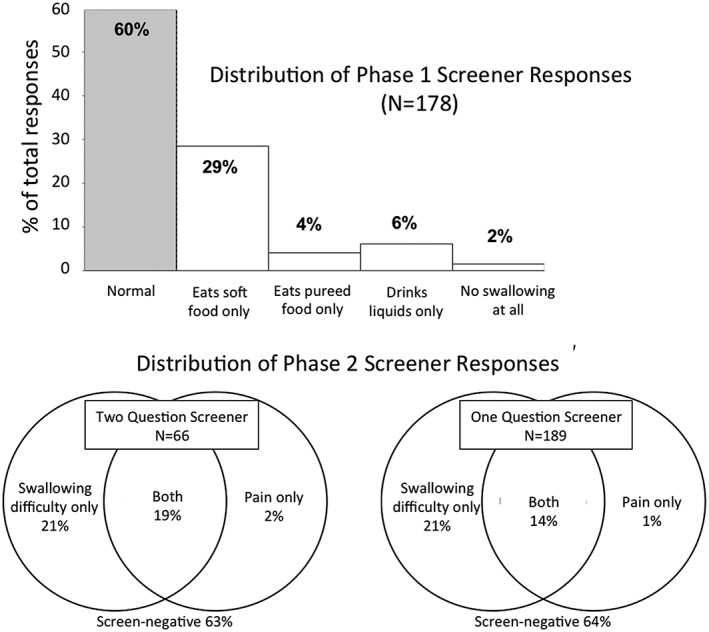
In Phase 1 (n = 178 esophageal cancer patients), the screening question "How are you currently eating?" had the highest sensitivities and specificities against various Swallowing Index Cut-Off Value cut-offs, with the best optimal cutoff associated with weight loss (80% sensitivity and 75% specificity). In phase 2 (255 head and neck, gastro-esophageal, and thoracic cancer patients), a single question screener ("Do you experience any difficulty or pain upon swallowing?") versus a Patient Reported Outcomes for Common Terminology Criteria for Adverse Events-like gold standard generated sensitivities between 86% and 94% and specificities between 93% and 100%. This screening question (+/- follow-up questions) had a median completion time of under 2 minutes, and >90% of patients were willing to complete the survey electronically, did not feel that survey made clinic visit more difficult, and did not find the questions upsetting or distressful.
Our results demonstrate that these screener tools ("How are you currently eating?", "Do you experience any difficulty or pain upon swallowing?") can effectively screen dysphagia symptoms without increasing cancer outpatient clinic burden, both in observational studies and for routine clinical monitoring.
吞咽困难可能与癌症患者的严重发病情况相关。我们旨在开发并评估用于观察性研究(第1阶段)以及临床护理中常规症状监测(第2阶段)的吞咽困难筛查工具。
在一个专家小组对内容、标准和结构效度进行审查后,挑选出各种吞咽困难或吞咽疼痛筛查问题,并将其与癌症治疗功能评估-食管癌(FACT-E)吞咽指数临界值或根据不良事件通用术语标准的患者报告结局改编的问题进行比较。评估了敏感性、特异性和患者可接受性。
在第1阶段(n = 178例食管癌患者),筛查问题“你目前进食情况如何?”针对各种吞咽指数临界值具有最高的敏感性和特异性,与体重减轻相关的最佳最佳临界值具有80%的敏感性和75%的特异性。在第2阶段(255例头颈部、胃食管和胸段癌症患者),一个单一问题筛查器(“你吞咽时是否有任何困难或疼痛?”)与一个类似不良事件通用术语标准的患者报告结局金标准相比,敏感性在86%至94%之间,特异性在93%至100%之间。这个筛查问题(±后续问题)的中位完成时间不到2分钟,超过90%的患者愿意以电子方式完成调查,不觉得调查使门诊就诊更困难,也不觉得问题令人不安或痛苦。
我们的结果表明,这些筛查工具(“你目前进食情况如何?”,“你吞咽时是否有任何困难或疼痛?”)在观察性研究和常规临床监测中都能有效筛查吞咽困难症状,而不会增加癌症门诊负担。