Pfaff Colin, Singano Victor, Akello Harriet, Amberbir Alemayehu, Berman Josh, Kwekwesa Aunex, Matengeni Alfred, Banda Victor, Msonko Jack, Speight Colin, Kabeya Biselele M, van Oosterhout Joep J
Dignitas International, Zomba, Malawi.
Department of Family Medicine, College of Medicine, University of Malawi, Blantyre, Malawi.
Malawi Med J. 2018 Sep;30(3):211-214. doi: 10.4314/mmj.v30i3.14.
Malawi has the highest rate of cervical cancer globally and cervical cancer is six to eight times more common in women with HIV. HIV programmes provide an ideal setting to integrate cervical cancer screening.
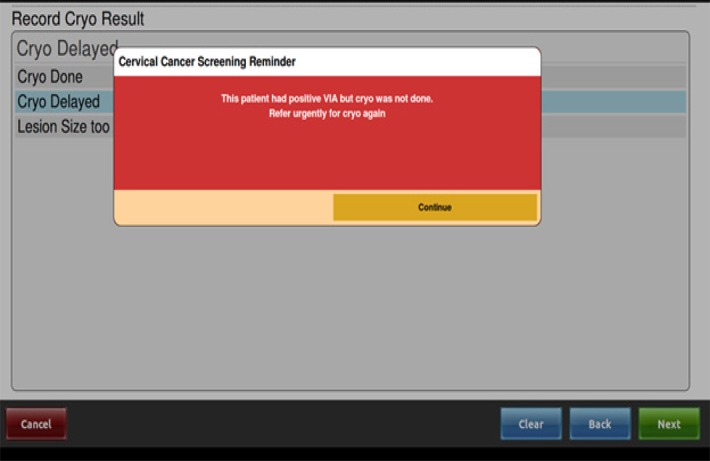
Tisungane HIV clinic at Zomba Central Hospital has around 3,700 adult women receiving treatment. In October 2015, a model of integrated cervical cancer screening using visual inspection with acetic acid (VIA) was adopted. All women aged 20 and above in the HIV clinic were asked if they had cervical cancer screening in the past three years and, if not, were referred for screening. Screening was done daily by nurses in a room adjacent to the HIV clinic. Cold coagulation was used to treat pre-cancerous lesions. From October 2016, a modification to the HIV programme's electronic medical record was developed that assisted in matching numbers of women sent for screening with daily screening capacity and alerted providers to women with pre-cancerous lesions who missed referrals or treatment.
Between May 2016 and March 2017, cervical cancer screening was performed in 957 women from the HIV clinic. Of the 686 (71%) women who underwent first ever screening, 23 (3.4%) were found to have VIA positive lesions suggestive of pre-cancer, of whom 8 (35%) had a same-day cold coagulation procedure, seven (30%) deferred cold coagulation to a later date (of whom 4 came for treatment), and 8 (35%) were referred to surgery due to size of lesion; 5/686 (0.7%) women had lesions suspicious of cancer.
Incorporating cervical cancer screening into services at HIV clinics is feasible. A structured approach to screening in the HIV clinic was important.
马拉维是全球宫颈癌发病率最高的国家,且感染艾滋病毒的女性患宫颈癌的几率要高6至8倍。艾滋病毒防治项目为整合宫颈癌筛查提供了理想环境。
松巴中央医院的Tisungane艾滋病毒诊所约有3700名成年女性接受治疗。2015年10月,该诊所采用了醋酸目视检查(VIA)这一综合宫颈癌筛查模式。诊所询问了所有20岁及以上的女性在过去三年是否接受过宫颈癌筛查,若未接受,则转介她们进行筛查。筛查工作由护士在艾滋病毒诊所隔壁的房间每天进行。采用冷凝法治疗癌前病变。从2016年10月起,对艾滋病毒防治项目的电子病历进行了修改,以协助将送去筛查的女性人数与每日筛查能力相匹配,并提醒医护人员注意那些错过转介或治疗的癌前病变女性。
2016年5月至2017年3月期间,艾滋病毒诊所的957名女性接受了宫颈癌筛查。在686名(71%)首次接受筛查的女性中,23名(3.4%)被发现醋酸目视检查呈阳性,提示有癌前病变,其中8名(35%)当天接受了冷凝治疗,7名(30%)推迟到日后进行冷凝治疗(其中4名前来接受治疗),8名(35%)因病变大小被转介接受手术;5/686(0.7%)的女性有疑似癌症的病变。
将宫颈癌筛查纳入艾滋病毒诊所的服务是可行的。在艾滋病毒诊所采用结构化的筛查方法很重要。