School of Medical Informatics, China Medical University, Shenyang, Liaoning, China.
Department of Medical Oncology, The First Hospital of China Medical University, Shenyang, 110001, Liaoning, China.
Eur Radiol. 2019 May;29(5):2388-2398. doi: 10.1007/s00330-018-5912-2. Epub 2019 Jan 14.
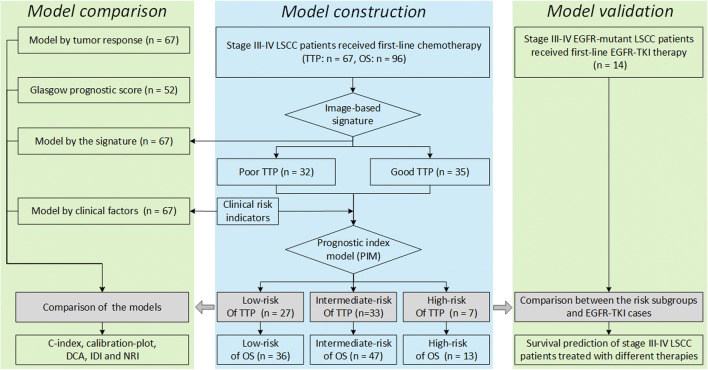
To establish a pre-therapy prognostic index model (PIM) of the first-line chemotherapy aiming to achieve accurate prediction of time to progression (TTP) and overall survival among the patients diagnosed with locally advanced (stage III) or distant metastasis (stage IV) lung squamous cell carcinoma (LSCC).
Ninety-six LSCC patients treated with first-line chemotherapy were retrospectively enrolled to build the model. Fourteen epidermal growth factor receptor (EGFR)-mutant LSCC patients treated with first-line EGFR-tyrosine kinase inhibitor (TKI) therapy were enrolled for validation dataset. From CT images, 56,000 phenotype features were initially computed. PIM was constructed by integrating a CT phenotype signature selected by the least absolute shrinkage and selection operator and the significant blood-based biomarkers selected by multivariate Cox regression. PIM was then compared with other four prognostic models constructed by the CT phenotype signature, clinical factors, post-therapy tumor response, and Glasgow Prognostic Score.
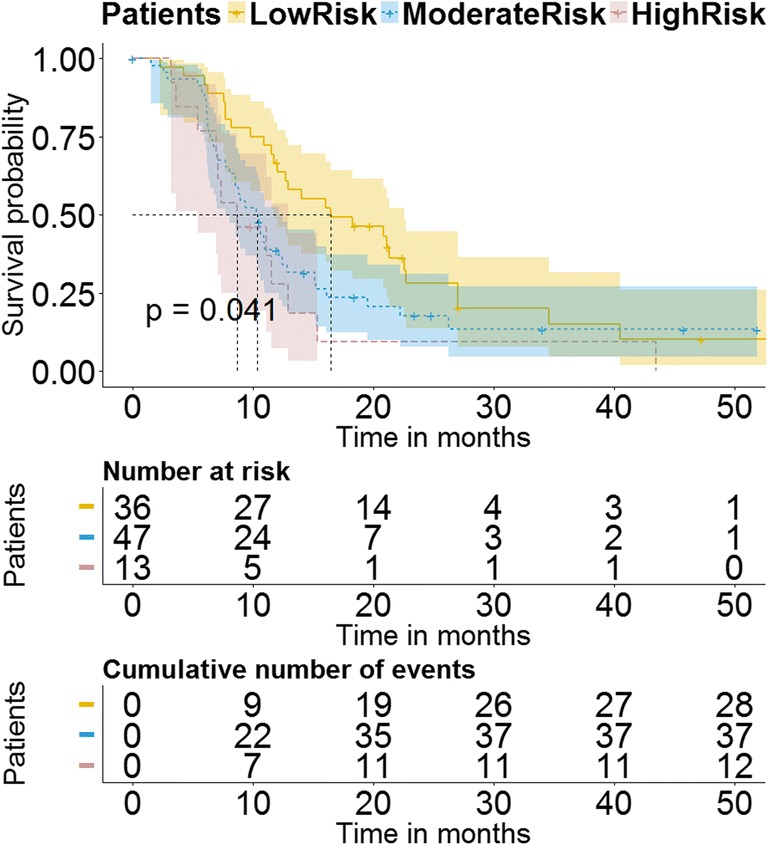
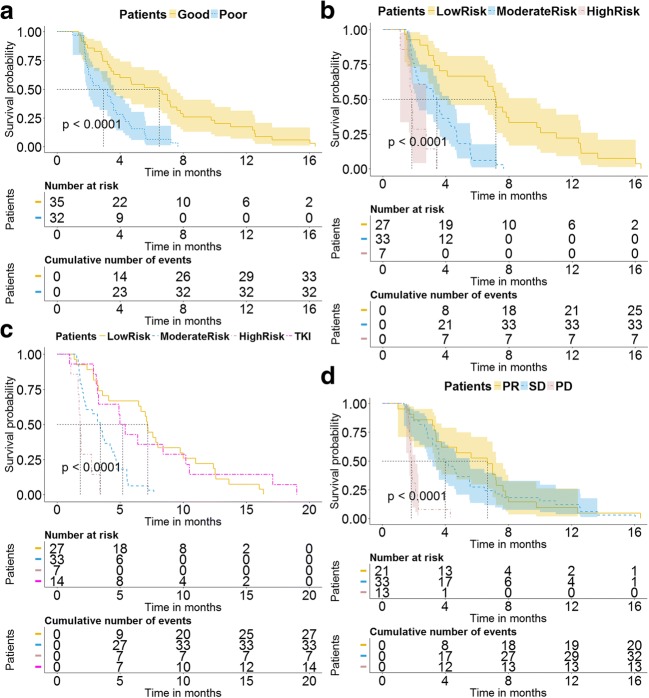
The signature includes eight optimal features extracted from co-occurrence, run length, and Gabor features. By using PIM, chemotherapy efficacy of patients categorized in the low-risk, intermediate-risk, and high-risk progression subgroups (median TTP = 7.2 months, 3.4 months, and 1.8 months, respectively) was significantly different (p < 0.0001, log-rank test). Chemotherapy efficacy of the low-risk progression subgroup was comparable with EGFR-TKI therapy (p = 0.835, log-rank test). Prognostic prediction of chemotherapy efficacy by PIM was significantly higher than other models (p < 0.05, z test).
The study demonstrated that the PIM yielded significantly higher performance to identify individual stage III-IV LSCC patients who can potentially benefit most from first-line chemotherapy, and predict the risk of failure from chemotherapy for individual patients.
• TTP and OS of first-line chemotherapy in individual stage III-IV LSCC patients could be predicted by pre-therapy blood-based biomarkers and image-based signatures. • Risk status of pre-therapy indicators affected the efficacy of first-line chemotherapy in stage III-IV LSCC patients. • Those stage III-IV LSCC patients who were able to achieve similar efficacy to EGFR-TKI therapy through chemotherapy were identified.
建立一线化疗的治疗前预后指数模型(PIM),旨在准确预测局部晚期(III 期)或远处转移(IV 期)肺鳞状细胞癌(LSCC)患者的疾病进展时间(TTP)和总生存期。
回顾性纳入 96 例接受一线化疗的 LSCC 患者建立模型。纳入 14 例接受一线表皮生长因子受体(EGFR)突变 LSCC 患者接受一线 EGFR 酪氨酸激酶抑制剂(TKI)治疗的患者作为验证数据集。从 CT 图像中,最初计算了 56,000 个表型特征。通过整合由最小绝对收缩和选择算子选择的 CT 表型特征和由多元 Cox 回归选择的显著血液生物标志物来构建 PIM。然后,将 PIM 与通过 CT 表型特征、临床因素、治疗后肿瘤反应和格拉斯哥预后评分构建的其他四个预后模型进行比较。
该特征包括从共现、运行长度和 Gabor 特征中提取的八个最佳特征。使用 PIM,在低风险、中风险和高风险进展亚组中,患者的化疗疗效(中位 TTP=7.2 个月、3.4 个月和 1.8 个月)有显著差异(p<0.0001,对数秩检验)。低风险进展亚组的化疗疗效与 EGFR-TKI 治疗相当(p=0.835,对数秩检验)。PIM 对化疗疗效的预后预测明显优于其他模型(p<0.05,z 检验)。
该研究表明,PIM 可显著提高识别最有可能从一线化疗中获益的个体 III-IV 期 LSCC 患者的性能,并预测个体患者化疗失败的风险。
TTP 和 OS 可通过个体 III-IV 期 LSCC 患者的一线化疗前血生物标志物和图像特征来预测。
治疗前指标的风险状况影响 III-IV 期 LSCC 患者一线化疗的疗效。
确定了能够通过化疗达到与 EGFR-TKI 治疗相似疗效的 III-IV 期 LSCC 患者。