Division of Cardiovascular Medicine, Roy and Lucille J. Carver College of Medicine, University of Iowa Hospitals and Clinics, Iowa City.
Department of Internal Medicine, Roy and Lucille J. Carver College of Medicine, University of Iowa, Iowa City.
JAMA Netw Open. 2018 Sep 7;1(5):e182870. doi: 10.1001/jamanetworkopen.2018.2870.
Comparative effectiveness and safety of oral anticoagulants in patients with atrial fibrillation (AF) and multiple chronic conditions (MCC) are unknown.
To determine whether there are differences in efficacy and safety of dabigatran, rivaroxaban, and warfarin regarding stroke prevention and bleeding rates, respectively, in elderly patients with AF with MCC.
DESIGN, SETTING, AND PARTICIPANTS: This retrospective comparative effectiveness analysis included data from the population-based Medicare beneficiaries database, evaluating patients with new AF diagnosed from January 1, 2010, to December 31, 2013, who initiated an oral anticoagulant within 90 days of diagnosis. Patients with CHA2DS2-VASc scores of 1 to 3, 4 to 5, and 6 or higher; HAS-BLED scores of 0 to 1, 2, and 3 or higher; and Gagne comorbidity scores of 0 to 2, 3 to 4, and 5 or higher were categorized as having low, moderate, or high morbidity, respectively. Within morbidity categories, patients receiving dabigatran, rivaroxaban, or warfarin were matched using a 3-way propensity matching, and the relative hazards of stroke, major hemorrhage (MH), and death were evaluated. Data analysis included follow-up from the date of initial anticoagulant use through December 31, 2013.
Rivaroxaban (20 mg once daily), dabigatran (150 mg twice daily), or warfarin therapy.
Ischemic stroke, MH, and death.
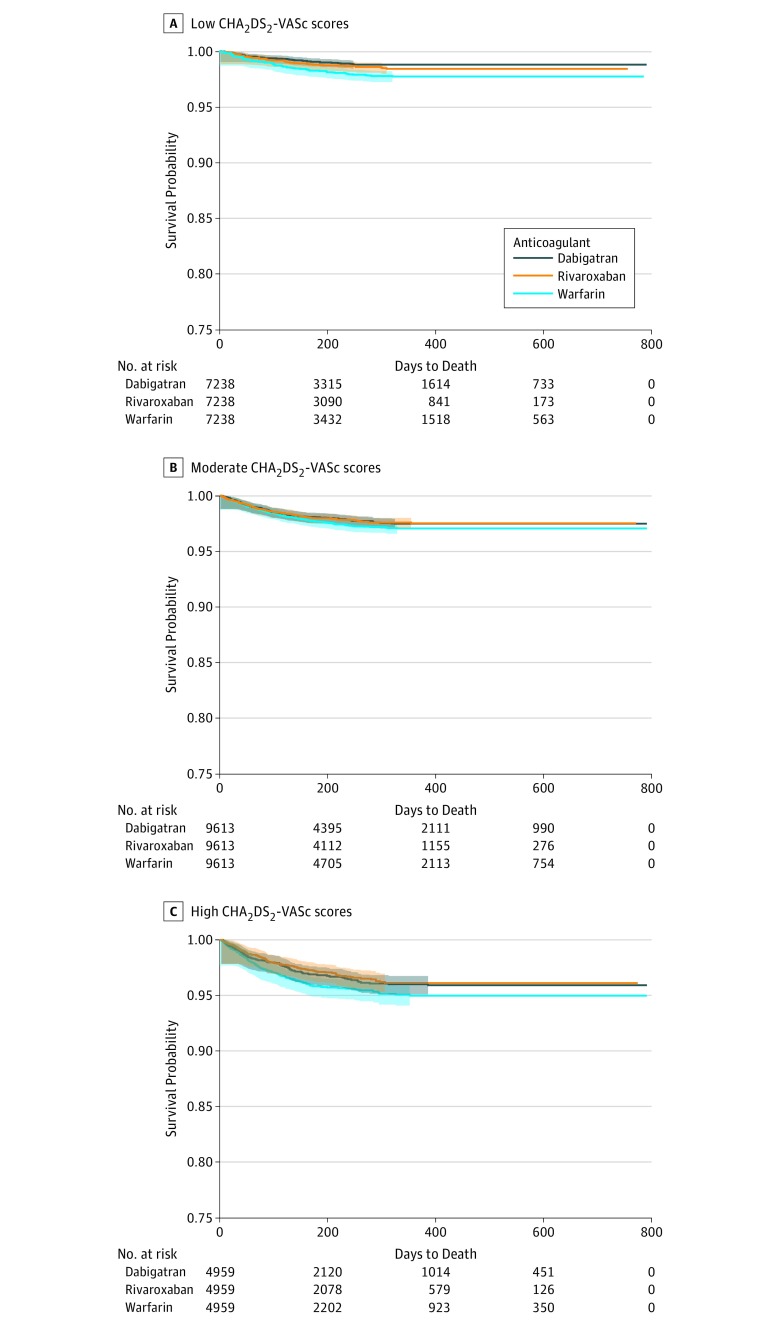
The study cohort included 21 979 patients using dabigatran (mean [SD] age, 75.8 [6.4] years; 51.1% female), 23 177 using rivaroxaban (mean [SD] age, 75.8 [6.4] years; 49.9% female), and 101 715 using warfarin (mean [SD] age, 78.5 [7.2] years; 57.3% female). In the propensity-matched cohorts, there were no differences in stroke rates between the 3 oral anticoagulant groups. Dabigatran users had lower hazard of MH compared with warfarin users among patients with low MCC (hazard ratio [HR], 0.62; 95% CI, 0.47-0.83; P < .001; for MCC defined as low CHA2DS2-VASc score), and similar risk in patients with moderate to high MCC. While there was no difference in MH between rivaroxaban and warfarin users, rivaroxaban users had significantly higher MH risk compared with dabigatran users in the medium and high comorbidity groups (HR, 1.24; 95% CI, 1.04-1.48; P = .02 and HR, 1.28; 95% CI, 1.05-1.56; P = .01, respectively). Dabigatran and rivaroxaban users had lower rates of death compared with warfarin users (HR ranged from 0.52-0.84), across comorbidity levels.
Oral anticoagulants are similarly effective in stroke prevention among patients with AF with MCC. However, dabigatran and rivaroxaban use may be associated with lower rates of mortality in patients with MCC.
在患有多种慢性疾病(MCC)的心房颤动(AF)患者中,口服抗凝剂的疗效和安全性比较尚不清楚。
确定在患有 MCC 的老年 AF 患者中,达比加群、利伐沙班和华法林在预防中风和出血率方面的疗效和安全性是否存在差异。
设计、设置和参与者:本回顾性比较有效性分析包括来自基于人群的 Medicare 受益人群数据库的数据,评估 2010 年 1 月 1 日至 2013 年 12 月 31 日期间新诊断为 AF 的患者,在诊断后 90 天内开始口服抗凝剂。CHA2DS2-VASc 评分 1 至 3、4 至 5 和 6 或更高;HAS-BLED 评分 0 至 1、2 和 3 或更高;以及 Gagne 合并症评分 0 至 2、3 至 4 和 5 或更高的患者分别归类为低、中、高发病率。在每个发病率类别内,通过 3 路倾向匹配,使用达比加群、利伐沙班或华法林的患者进行匹配,并评估中风、大出血(MH)和死亡的相对危险度。数据分析包括从初始抗凝治疗开始至 2013 年 12 月 31 日的随访。
利伐沙班(20mg 每日一次)、达比加群(150mg 每日两次)或华法林治疗。
缺血性中风、MH 和死亡。
研究队列包括使用达比加群的 21979 名患者(平均[标准差]年龄 75.8[6.4]岁;51.1%为女性)、使用利伐沙班的 23177 名患者(平均[标准差]年龄 75.8[6.4]岁;49.9%为女性)和使用华法林的 101715 名患者(平均[标准差]年龄 78.5[7.2]岁;57.3%为女性)。在倾向匹配的队列中,3 种口服抗凝剂组之间的中风发生率无差异。在 MCC 低发病率患者中,与华法林使用者相比,达比加群使用者 MH 的风险较低(危险比[HR],0.62;95%CI,0.47-0.83;P<0.001;MCC 定义为低 CHA2DS2-VASc 评分),在中至高 MCC 患者中风险相似。虽然 MH 率在利伐沙班和华法林使用者之间没有差异,但在中高合并症组中,利伐沙班使用者的 MH 风险明显高于达比加群使用者(HR,1.24;95%CI,1.04-1.48;P=0.02 和 HR,1.28;95%CI,1.05-1.56;P=0.01,分别)。与华法林使用者相比,达比加群和利伐沙班使用者的死亡率较低(HR 范围为 0.52-0.84),无论合并症水平如何。
在患有 MCC 的 AF 患者中,口服抗凝剂在预防中风方面同样有效。然而,达比加群和利伐沙班的使用可能与 MCC 患者的死亡率降低有关。