Department of Otolaryngology-Head and Neck surgery, Baylor College of Medicine, Houston, TX, USA.
Interdepartmental Program in Translational Biology and Molecular Medicine, Baylor College of Medicine, Houston, TX, USA.
J Immunother Cancer. 2019 Jan 15;7(1):10. doi: 10.1186/s40425-018-0485-9.
Chemoradiotherapy (CRT) remains one of the most common cancer treatment modalities, and recent data suggest that CRT is maximally effective when there is generation of an anti-tumoral immune response. However, CRT has also been shown to promote immunosuppressive mechanisms which must be blocked or reversed to maximize its immune stimulating effects.
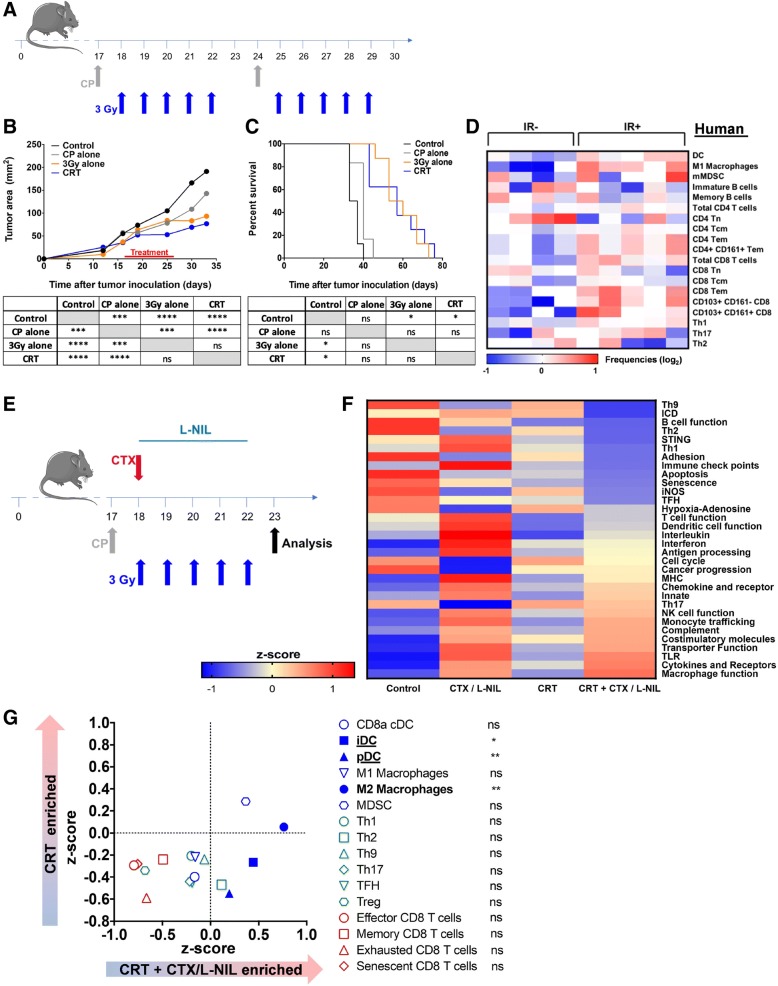
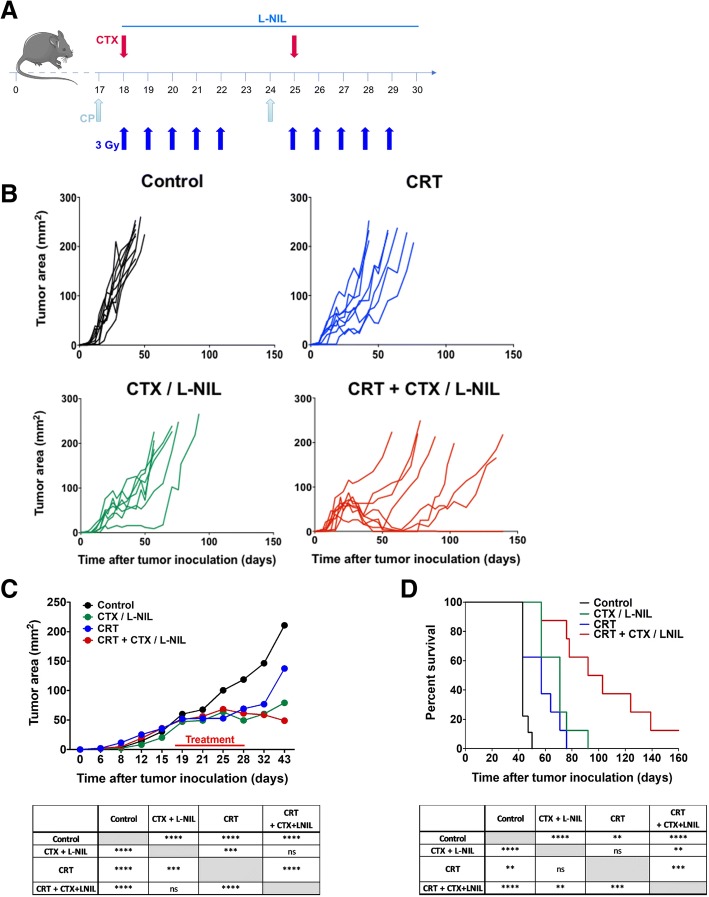
Therefore, using a preclinical model of human papillomavirus (HPV)-associated head and neck squamous cell carcinoma (HNSCC), we developed a clinically relevant therapy combining CRT and two existing immunomodulatory drugs: cyclophosphamide (CTX) and the small molecule inducible nitric oxide synthase (iNOS) inhibitor L-n6-(1-iminoethyl)-lysine (L-NIL). In this model, we treated the syngeneic HPV-HNSCC mEER tumor-bearing mice with fractionated (10 fractions of 3 Gy) tumor-directed radiation and weekly cisplatin administration. We compared the immune responses induced by CRT and those induced by combinatory treatment (CRT + CTX/L-NIL) with flow cytometry, quantitative multiplex immunofluorescence and by profiling immune-related gene expression changes.
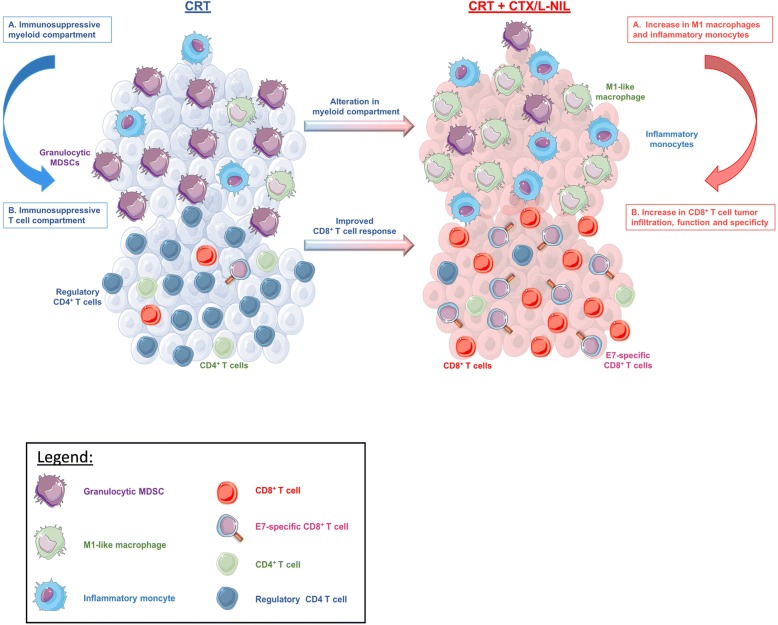
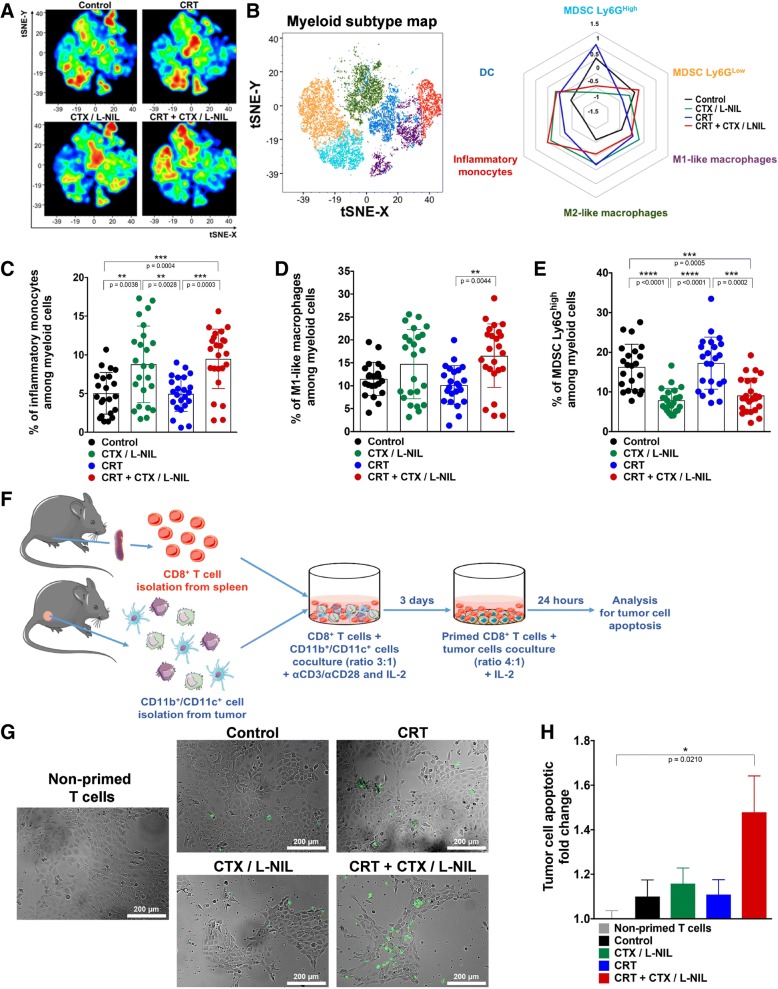
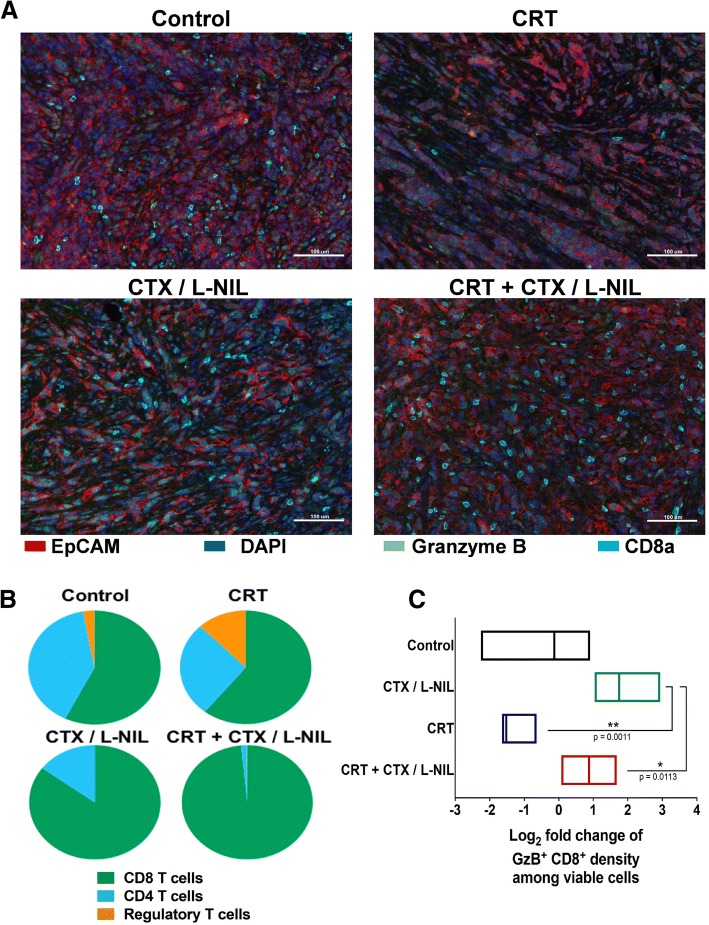
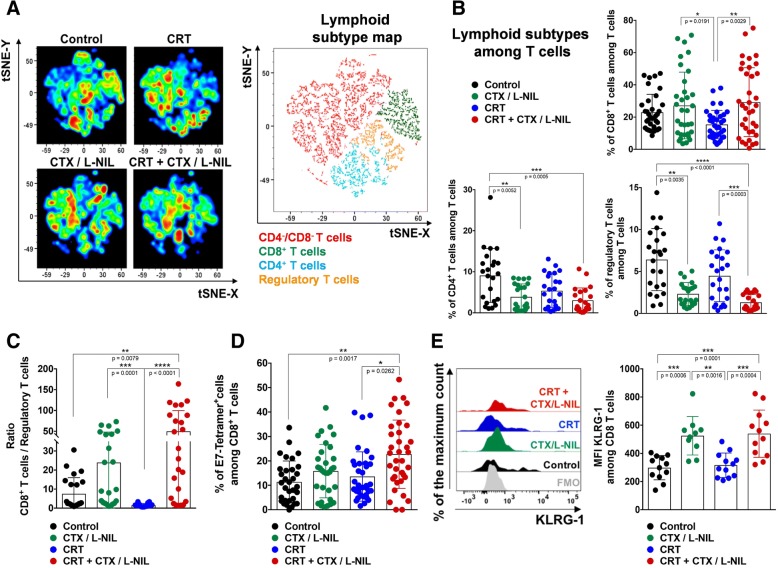
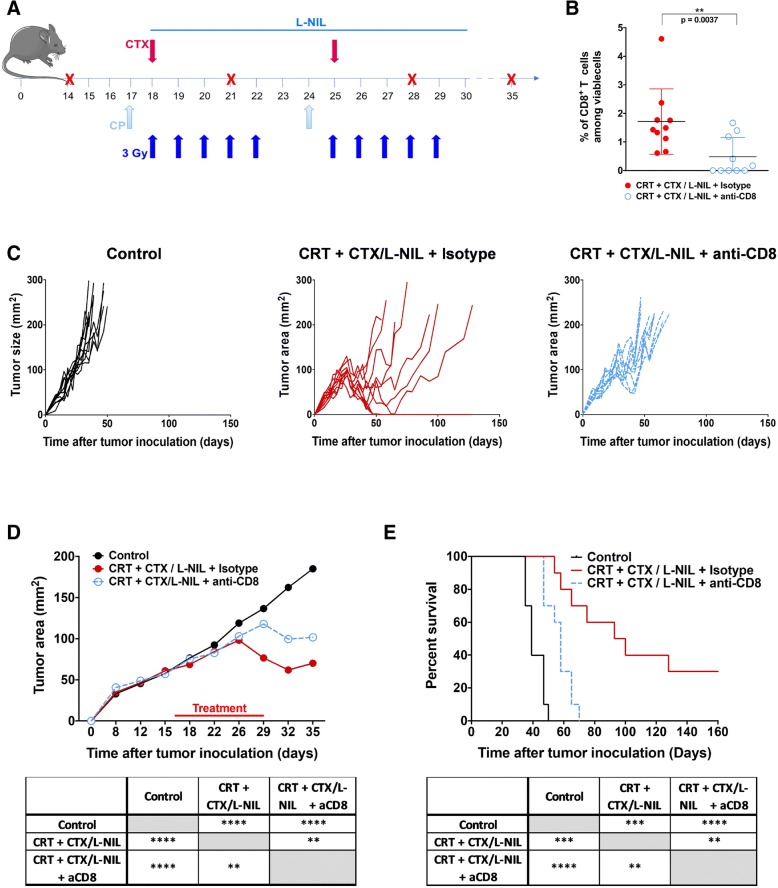
We show that combination treatment favorably remodels the tumor myeloid immune microenvironment including an increase in anti-tumor immune cell types (inflammatory monocytes and M1-like macrophages) and a decrease in immunosuppressive granulocytic myeloid-derived suppressor cells (MDSCs). Intratumoral T cell infiltration and tumor antigen specificity of T cells were also improved, including a 31.8-fold increase in the CD8 T cell/ regulatory T cell ratio and a significant increase in tumor antigen-specific CD8 T cells compared to CRT alone. CTX/LNIL immunomodulation was also shown to significantly improve CRT efficacy, leading to rejection of 21% established tumors in a CD8-dependent manner.
Overall, these data show that modulation of the tumor immune microenvironment with CTX/L-NIL enhances susceptibility of treatment-refractory tumors to CRT. The combination of tumor immune microenvironment modulation with CRT constitutes a translationally relevant approach to enhance CRT efficacy through enhanced immune activation.
放化疗(CRT)仍然是最常见的癌症治疗方式之一,最近的数据表明,当产生抗肿瘤免疫反应时,CRT 的效果最佳。然而,CRT 也已被证明会促进免疫抑制机制,为了最大限度地发挥其免疫刺激作用,这些机制必须被阻断或逆转。
因此,我们使用人乳头瘤病毒(HPV)相关头颈部鳞状细胞癌(HNSCC)的临床前模型,开发了一种将 CRT 与两种现有的免疫调节药物相结合的临床相关疗法:环磷酰胺(CTX)和小分子诱导型一氧化氮合酶(iNOS)抑制剂 L-n6-(1-亚氨基乙基)-赖氨酸(L-NIL)。在该模型中,我们用分次(10 次 3Gy)肿瘤定向放射和每周顺铂给药治疗同源 HPV-HNSCC mEER 荷瘤小鼠。我们通过流式细胞术、定量多重免疫荧光和免疫相关基因表达变化谱分析比较 CRT 和联合治疗(CRT+CTX/L-NIL)诱导的免疫反应。
我们表明,联合治疗有利于重塑肿瘤髓样免疫微环境,包括增加抗肿瘤免疫细胞类型(炎症单核细胞和 M1 样巨噬细胞)和减少免疫抑制性粒细胞髓样来源抑制细胞(MDSCs)。肿瘤内 T 细胞浸润和 T 细胞的肿瘤抗原特异性也得到改善,包括 CD8 T 细胞/调节性 T 细胞比值增加 31.8 倍,与 CRT 单独治疗相比,肿瘤抗原特异性 CD8 T 细胞显著增加。CTX/LNIL 免疫调节还显示出显著提高 CRT 疗效的作用,导致以 CD8 依赖性方式拒绝 21%的已建立肿瘤。
总的来说,这些数据表明,CTX/L-NIL 调节肿瘤免疫微环境可增强治疗抵抗性肿瘤对 CRT 的敏感性。肿瘤免疫微环境调节与 CRT 的联合构成了一种具有转化相关性的方法,通过增强免疫激活来提高 CRT 的疗效。