Orozco Guillén Alejandra Oralia, Velazquez Silva Ricardo Ivan, Moguel González Bernardo, Guell Yubia Amaya, Garciadiego Fossas Pamela, Custodio Gómez Iris Guadalupe, Miranda Araujo Osvaldo, Soto Abraham Virgilia, Piccoli Giorgina Barbara, Madero Magdalena
Department of Nephrology, National Institute of Perinatology "Isidro Espinoza de los Reyes", Mexico City 11000, Mexico.
Department of Nephrology, National Institute of Cardiology "Ignacio Chávez", Mexico City 14080, Mexico.
J Clin Med. 2019 Jan 18;8(1):114. doi: 10.3390/jcm8010114.
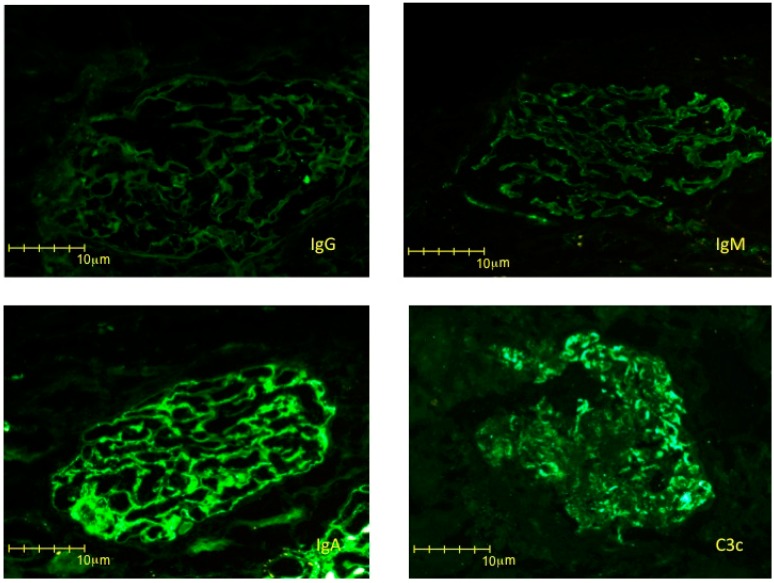
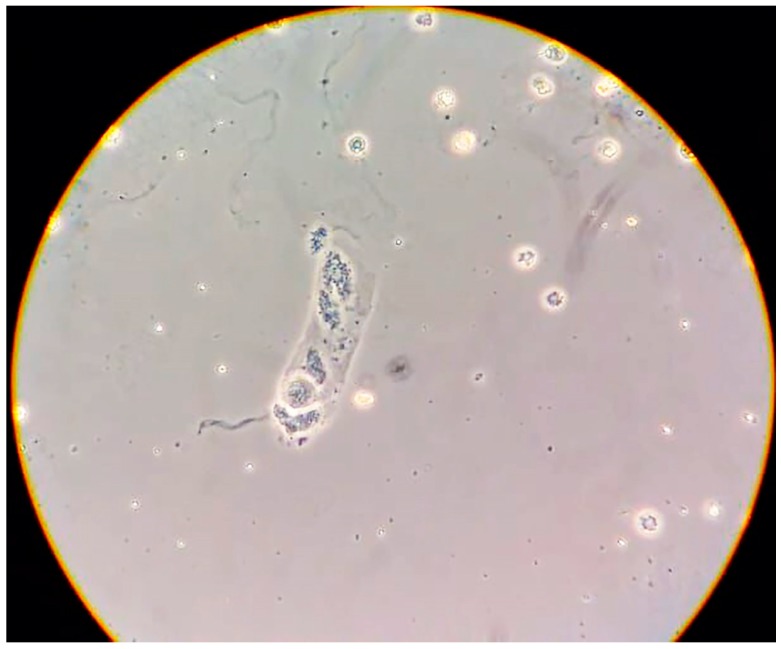
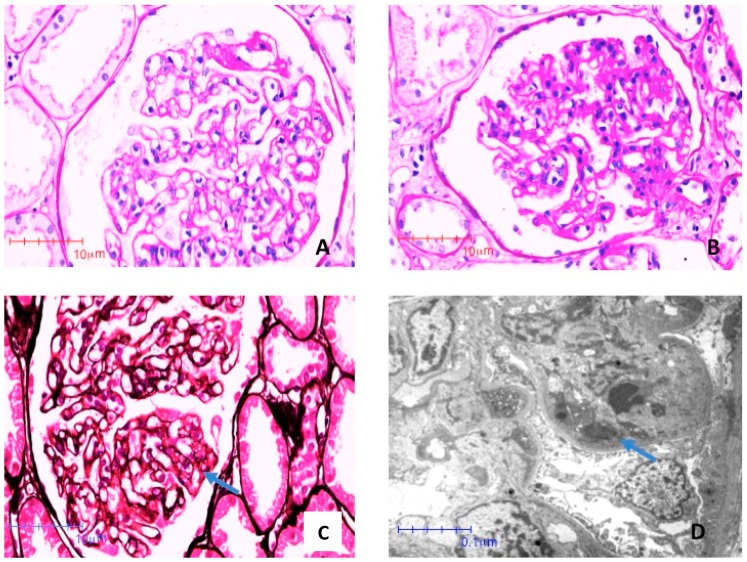
Chronic kidney disease (CKD) is increasingly recognized as a risk factor in pregnancy; the differential diagnosis between CKD and preeclampsia (PE) may be of pivotal importance for pregnancy management and for early treatment of CKD. Acknowledging this connection may be useful also in a wider context, such as in the case reported in this paper, which for the first time describes an association between syphilis infection and IgA-dominant glomerulonephritis. A 16-year-old woman, referred to a general hospital due to a seizure, was found to be unknowingly pregnant. Based on hypertension and nephrotic proteinuria, she was initially diagnosed with PE. Immunological tests, as well as hepatitis and HIV tests showed negative results. However, secondary syphilis was diagnosed. In discordance with the PE diagnosis, urinalysis showed glomerular microhematuria with cellular casts. Proteinuria and hypertension did not remit after delivery, which was made via caesarean section, due to uncontrolled hypertension, at an estimated gestational age of 29 weeks. A male baby, weighing 1.1 kg (6.5 centile) was born. The baby was hospitalized in the neonatal intensive care unit, where he developed subependymal hemorrhage and thrombocytopenia, and neonatal syphilis was diagnosed. The mother underwent a kidney biopsy one week after delivery, leading to the diagnosis of IgA-dominant postinfectious glomerulonephritis. Mother and child were treated with support and antibiotic therapy, and were discharged in good clinical conditions four weeks later. Four months after delivery, the mother was normotensive without therapy, with normal kidney function and without hematuria or proteinuria. In conclusion, this case suggests that IgA-dominant postinfectious glomerulonephritis should be added to the spectrum of syphilis-associated glomerulonephritides, and underlines the need for a careful differential diagnosis with CKD in all cases of presumed PE. While diagnosis relies on kidney biopsy, urinary sediment, a simple and inexpensive test, can be the first step in distinguishing PE from other nephropathies.
慢性肾脏病(CKD)日益被视为妊娠的一个风险因素;CKD与子痫前期(PE)的鉴别诊断对于妊娠管理和CKD的早期治疗可能至关重要。认识到这种关联在更广泛的背景下也可能有用,例如在本文报道的病例中,该病例首次描述了梅毒感染与IgA主导的肾小球肾炎之间的关联。一名16岁女性因癫痫发作被转诊至综合医院,结果发现她已在不知情的情况下怀孕。基于高血压和肾病性蛋白尿,她最初被诊断为PE。免疫检查以及肝炎和HIV检测结果均为阴性。然而,诊断出二期梅毒。与PE诊断不一致的是,尿液分析显示肾小球性镜下血尿伴细胞管型。由于高血压未得到控制,在估计孕周29周时通过剖宫产分娩后,蛋白尿和高血压并未缓解。一名体重1.1千克(第6.5百分位)的男婴出生。婴儿入住新生儿重症监护病房,在那里他出现了室管膜下出血和血小板减少症,并被诊断为新生儿梅毒。母亲在分娩一周后接受了肾活检,结果诊断为IgA主导的感染后肾小球肾炎。母婴接受了支持治疗和抗生素治疗,四周后临床状况良好出院。分娩四个月后,母亲未经治疗血压正常,肾功能正常,无血尿或蛋白尿。总之,该病例表明IgA主导的感染后肾小球肾炎应被纳入梅毒相关肾小球肾炎的范畴,并强调在所有疑似PE病例中都需要与CKD进行仔细的鉴别诊断。虽然诊断依赖于肾活检,但尿沉渣检查作为一种简单且廉价的检测方法,可以作为区分PE与其他肾病的第一步。