Department of Internal Medicine, Erasmus University Medical Center, Rotterdam, the Netherlands.
Department of Emergency Medicine, Erasmus University Medical Center, Rotterdam, the Netherlands.
PLoS One. 2019 Jan 25;14(1):e0211133. doi: 10.1371/journal.pone.0211133. eCollection 2019.
In hospitalized patients, the risk of sepsis-related mortality can be assessed using the quick Sepsis-related Organ Failure Assessment (qSOFA). Currently, different tools that predict deterioration such as the National Early Warning Score (NEWS) have been introduced in clinical practice in Emergency Departments (ED) worldwide. It remains ambiguous which screening tool for mortality at the ED is best. The objective of this study was to evaluate the predictive performance for mortality of two sepsis-based scores (i.e. qSOFA and Systemic Inflammatory Response Syndrome (SIRS)-criteria) compared to the more general NEWS score, in patients with suspected infection directly at presentation to the ED.
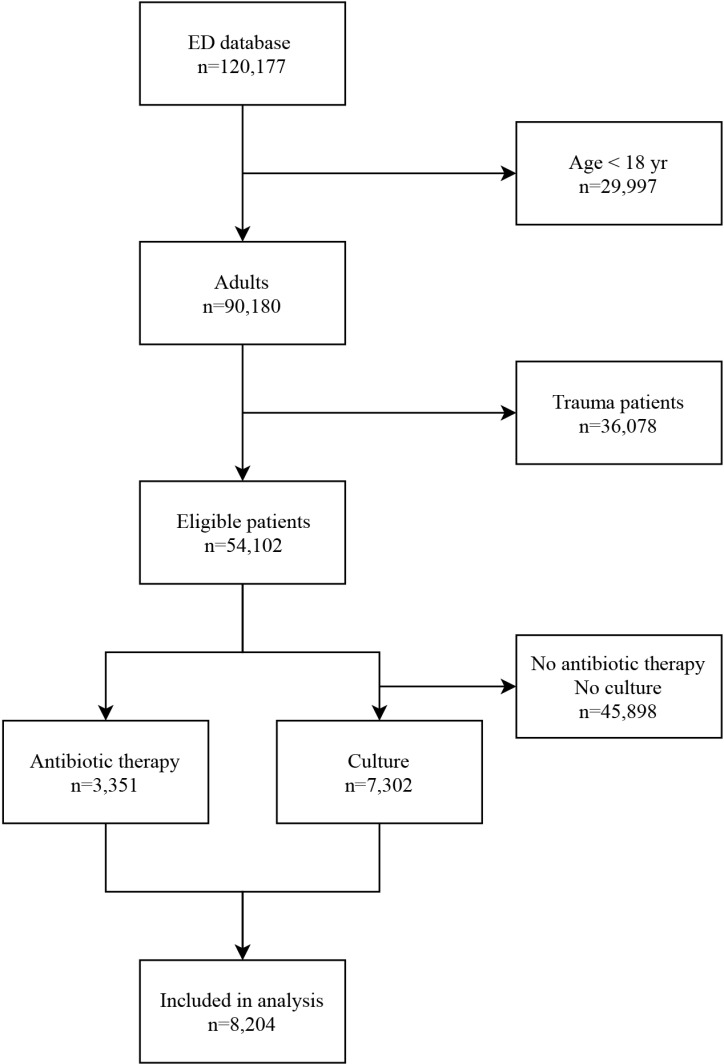
We performed a retrospective cohort study. Patients who presented to the ED between June 2012 and May 2016 with suspected sepsis in a large tertiary care center were included. Suspected sepsis was defined as initiation of intravenous antibiotics and/or collection of any culture in the ED. Outcome was defined as 10-day and 30-day mortality after ED presentation. Predictive performance was expressed as discrimination (AUC) and calibration using Hosmer-Lemeshow goodness-of-fit test. Subsequently, sensitivity, and specificity were calculated.
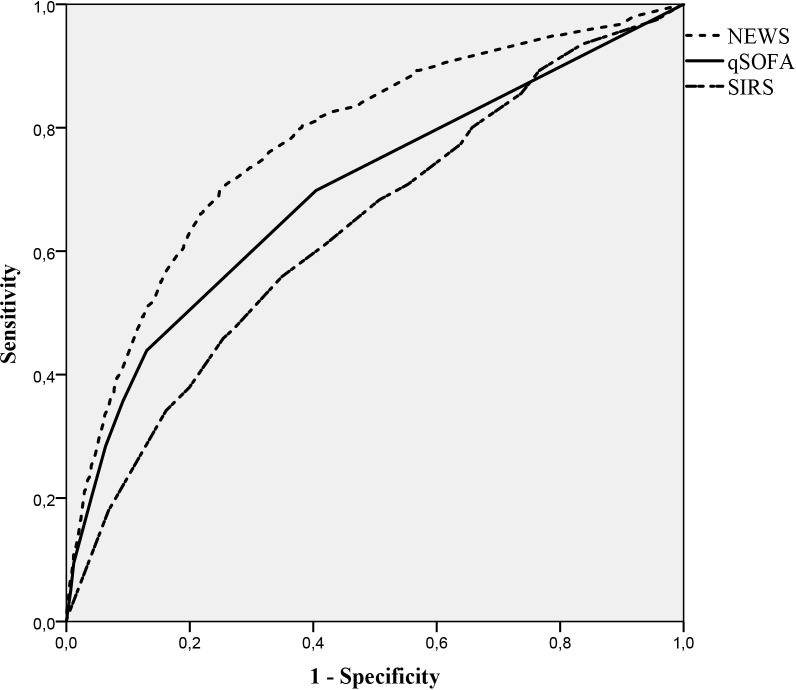
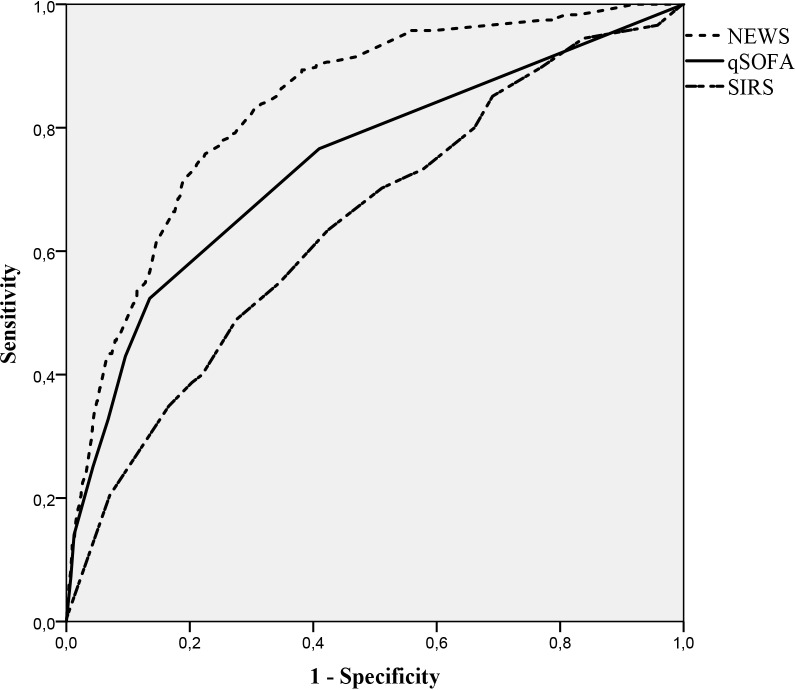
In total 8,204 patients were included of whom 286 (3.5%) died within ten days and 490 (6.0%) within 30 days after presentation. NEWS had the best performance, followed by qSOFA and SIRS (10-day AUC: 0.837, 0.744, 0.646, 30-day AUC: 0.779, 0.697, 0.631). qSOFA (≥2) lacked a high sensitivity versus SIRS (≥2) and NEWS (≥7) (28.5%, 77.2%, 68.0%), whilst entailing highest specificity versus NEWS and SIRS (93.7%, 66.5%, 37.6%).
NEWS is more accurate in predicting 10- and 30-day mortality than qSOFA and SIRS in patients presenting to the ED with suspected sepsis.
在住院患者中,可以使用快速脓毒症相关器官衰竭评估(qSOFA)评估与脓毒症相关的死亡风险。目前,在全球范围内,许多急诊部(ED)已经引入了不同的预测恶化的工具,如国家早期预警评分(NEWS)。哪种 ED 死亡率筛查工具最好仍不明确。本研究的目的是评估两种基于脓毒症的评分(即 qSOFA 和全身性炎症反应综合征(SIRS)标准)与更广泛的 NEWS 评分相比,在 ED 就诊时疑似感染的患者中对死亡率的预测性能。
我们进行了一项回顾性队列研究。纳入 2012 年 6 月至 2016 年 5 月期间在一家大型三级护理中心 ED 就诊疑似脓毒症的患者。疑似脓毒症的定义为在 ED 开始静脉使用抗生素和/或采集任何培养物。结局定义为 ED 就诊后 10 天和 30 天的死亡率。使用 Hosmer-Lemeshow 拟合优度检验来表示预测性能的区分度(AUC)和校准。随后计算了敏感性和特异性。
共纳入 8204 例患者,其中 286 例(3.5%)在 10 天内死亡,490 例(6.0%)在 30 天内死亡。NEWS 的性能最好,其次是 qSOFA 和 SIRS(10 天 AUC:0.837、0.744、0.646,30 天 AUC:0.779、0.697、0.631)。qSOFA(≥2)与 SIRS(≥2)和 NEWS(≥7)相比,敏感性较低(28.5%、77.2%、68.0%),而特异性较高(93.7%、66.5%、37.6%)。
在 ED 就诊疑似脓毒症的患者中,NEWS 预测 10 天和 30 天死亡率比 qSOFA 和 SIRS 更准确。